
EFM Pattern Recognition
Electronic fetal monitors continuously record the instantaneous fetal heart rate on the upper channel and uterine contractions on the lower channel. They do this by attaching, either externally (and non-invasively) or internally, to detect the fetal heart and each uterine contraction.

Labor is an inherently dangerous life event for a fetus and its mother. In the majority of cases, everything goes smoothly enough and ends happily. In a minority of cases, there are some problems. Electronic fetal monitoring is used to provide:
-
Minute-by-minute information on the status of the fetus
-
Accurate historical information on fetal status and the frequency/duration of contractions from earlier in labor.
-
Insight into the stresses on the fetus and its ability to tolerate those stresses.
Originally, electronic fetal monitoring was thought to be able to prevent such newborn problems as stillbirth, brain damage, seizure disorders, and cerebral palsy. This hope proved to be overly optimistic. Unfortunately, and contrary to earlier thinking, most of the problems that lead to stillbirth, brain damage, seizure disorders and cerebral palsy are not intrapartum problems, but have already occurred by the time a patient comes in to labor and delivery. Nonetheless, electronic fetal monitoring has proved so useful in so many ways that it has become a prominent feature of intrapartum care, and indispensable for high risk patients.
Two forms of continuous electronic fetal heart monitoring are used, internal and external. Internal monitoring provides the most accurate information, but requires a scalp electrode be attached to the fetus, and a pressure-sensing catheter to be inserted inside the uterine cavity. Both of these require membranes be ruptured and both have small, but not inconsequential risks. For that reason, they are usually used only when the clinical circumstances justify the small increased risk of complication.
External monitoring usually provides very good information about the timing of contractions and the fetal response. External monitoring consists of belts worn by the mother during labor that record the abdominal tension (indirectly recording a contraction), and the instantaneous fetal heart rate. External monitoring has the advantages of simplicity, safety, availability, and reasonable reliability under most general obstetrical circumstances. However, it is subject to more artifact than internal monitoring, may not detect subtle changes, and may not accurately record the information, particularly if the mother is overweight or active.
|
|
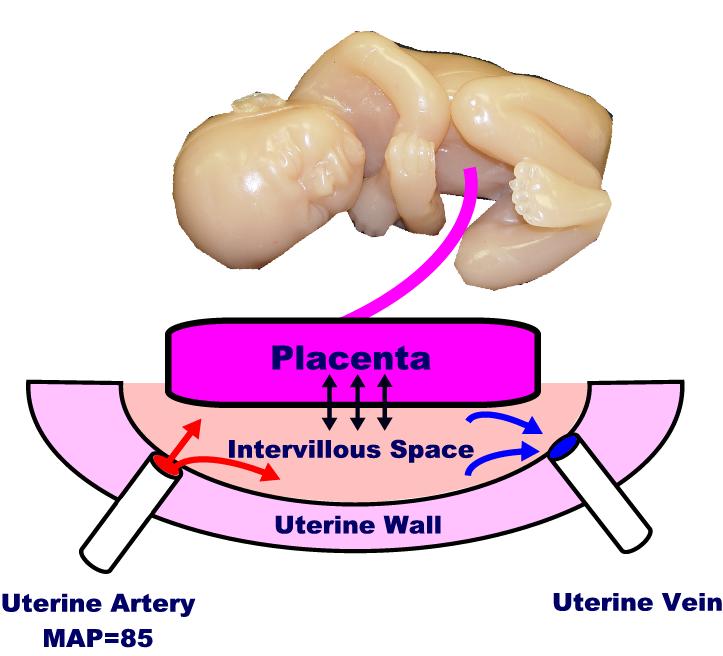
Maternal blood flows to the uterus primarily through the uterine arteries. The arteries branch out, once they enter the uterus, and supply blood to the muscle cells of the myometrium, and through the wall to the intervillous space (IVS). Once the maternal blood reaches the IVS, it simply dumped into the space, where it drifts about until some is drained off through the maternal venous system. Unlike the highly controlled capillary circulation, there is little control over this process. It is similar to a swimming pool (the IVS), where fresh water is dumped in through a faucet (the maternal arterioles), while the drains in the bottom of the pool (maternal venous system) sucks up any available water that happens to be nearby.
The placenta floats on top of the IVS, with its chorionic villi dipping down into the pool. Across the villous membrane pass oxygen, carbon dioxide, nutrients and waste products. Some of this passage is active transport (eg, glucose), some facilitated (eg, because of pH gradient), and some is passive.
Many factors influence uterine blood flow delivery to the IVS, including:
-
Maternal position (lateral, recumbant improves flow)
-
Maternal exercise (decreases flow)
-
Surface area of the placenta (placental abruption decreases flow)
-
Hypotension or hypertension (both decrease flow)
-
Uterine contractions (contractions reduce flow)
Once the maternal blood reaches the IVS, oxygen and nutrients must still must traverse the villous membrane. If thickened (as with edema or infection), then transvillous transport of materials will be impaired, at least to some degree.
Baseline Fetal Heart Rate
The baseline fetal heart rate is normally between 120 and 160 beats per minute (110 to 160 at full term). This seems to be the range that the normal, healthy fetus prefers to keep itself well-supplied with oxygen and nutrients. The heart can be faster, but only at a cost of increased energy utilization that is normally not justified. The heart can beat slower, but if the bradycardia is prolonged, it can lead to progressive tissue oxygen debt.
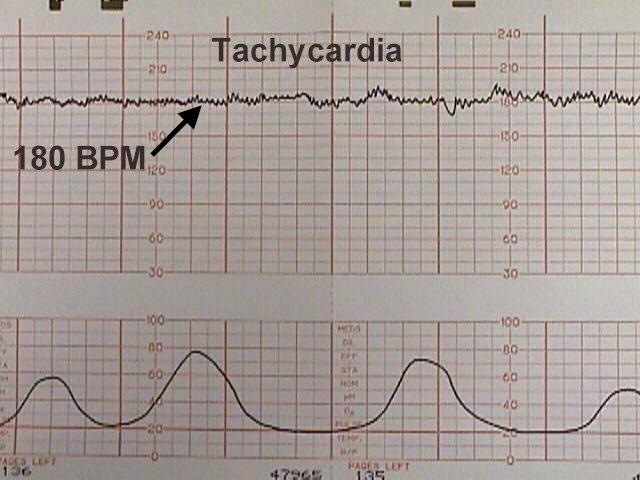 Tachycardia Tachycardia |
Tachycardia is the sustained elevation of fetal heart rate baseline above a 160 BPM. Tachycardia can be a normal response to some increased need for oxygen, for example:
-
Increased fetal activity (everyone’s heart rate goes up when we exercise)
-
Maternal fever (with an elevated body temperature, all enzyme systems speed up, increasing the need for oxygen on a metabolic basis)
It can also increase in the presence of more worrisome problems, including:
-
Chorioamnionitis
-
Maternal hypothyroidism
-
Drugs (Tocolytic drugs, Vistaril, etc.)
-
Fetal hypoxia
-
Fetal anemia
-
Fetal heart failure
-
Fetal arrhythmias
Most tachycardias are not indicative of fetal jeopardy, particularly in the absence of any other FHR abnormalities.
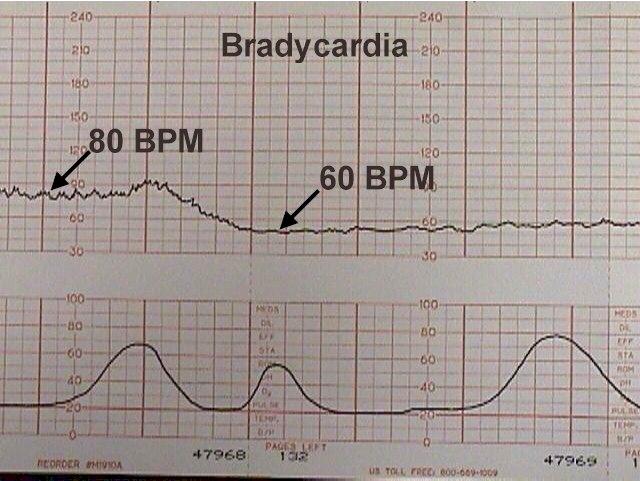  
Bradycardia |
Bradycardia is the sustained depression of fetal heart rate baseline below 120 BPM (110 at full term). Most of these are caused by increased vagal tone, although congenital cardiac abnormalities can also be responsible.
Mild bradycardia (to 80 or 90 BPM) with retention of beat-to-beat variability is common during the second stage of labor and not of great concern so long as delivery occurs relatively soon. Moderate to severe bradycardia (below 80 BPM) with loss of beat-to-beat variability, particularly in association with late decelerations, is more troubling and may indicate fetal distress, requiring prompt resolution.
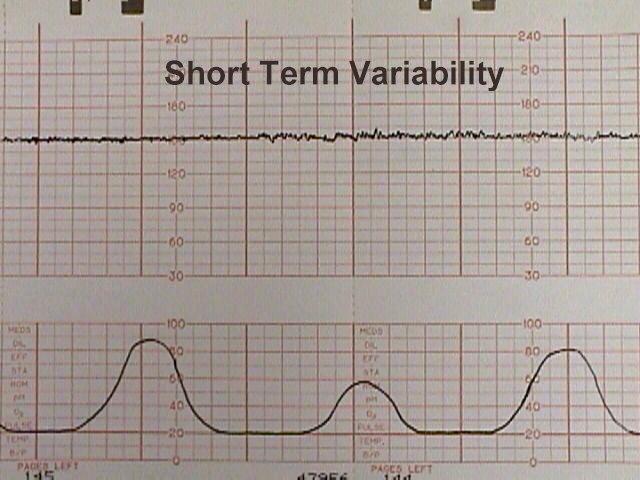
Variability
The normal fetal heart rate baseline is from 120 to 160 BPM and has both short and long-term “variability.” Short term variability means that from one moment to the next, the fetal heart speeds up slightly and then slows down slightly, usually with a range of 3-5 BPM from the baseline.
Variability is normally controlled by the fetal brain through sympathetic and parasympathetic influences. Reduced variability occurs normally during fetal sleep and usually returns after 20 to 40 minutes.
Reduced variability may also occur:
-
Following narcotic administration
-
With fetal anomalies or injury
-
With hypoxia and acidosis in combination with such FHR abnormalities as late decelerations, tachycardia, bradycardia, and severe variable decelerations.
Persistent or progressively reduced variability is not, by itself, a sign of fetal jeopardy. But in combination with other abnormalities may indicate fetal intolerance of labor.
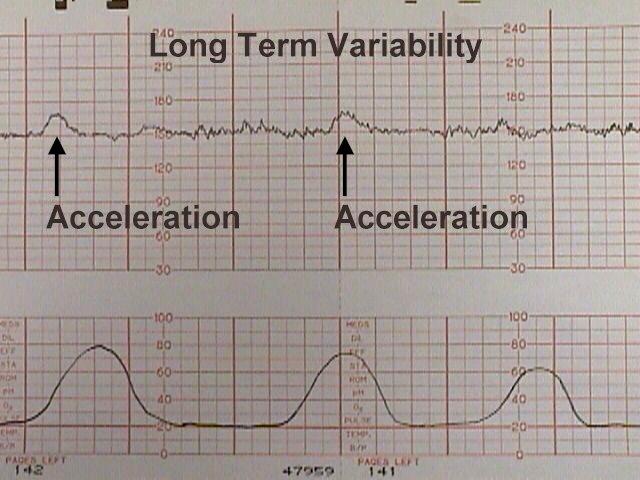
Long-term variability
Long-term variability represents broad-based swings in fetal heart rate, or “waviness,” occurring up to several times a minute. One form of long-term variability of particular significance is a fetal heart “acceleration.” These usually occur in response to fetal movement, and are 15 BPM above the baseline or more, lasting 10-20 seconds or longer. They can often be provoked by stimulating the fetal scalp during a pelvic examination, or by acoustically stimulating the fetus with a loud, obnoxious noise. The presence of fetal accelerations is reassuring that the fetus is healthy and tolerating the intrauterine environment well.
During labor, no significance is attached to the absence of fetal accelerations.
Effect of Contractions
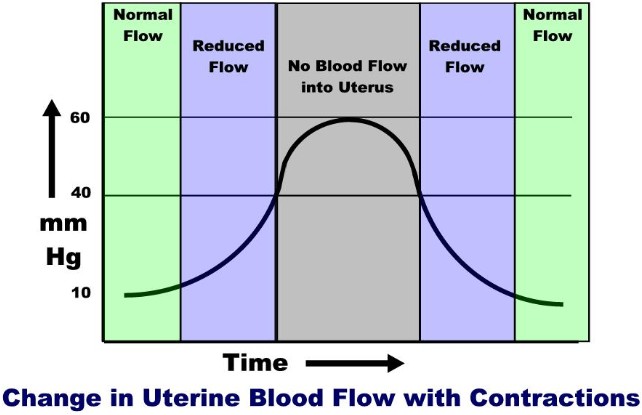
During a uterine contraction, blood flow through the uterus slows. If the contraction is strong enough, all blood flow through it will stop.
This decreased flow occurs because of the pressure gradients in the system.
Maternal mean arterial pressure (MAP) is around 85 mm Hg. The pressure on the inside of the uterus (at rest) is around 10 mm Hg. The pressure within the uterine muscle (intramyometrial pressure or IMP) is usually about 2-3 times that of the intra-amniotic pressure. Because of these pressures, blood flows from the high pressure uterine arteries, through the intramyometrial spiral arteries (and past the medium pressure intramyometrial zone) and into the low pressure intravillous space. From the IVS, blood is drained out through the even lower pressure venous system and returned to the mother’s circulation.
During a contraction, the intramyometrial pressures rise with the increased muscle tone. As the compressive pressure rises, blood flow through the spiral arteries diminishes (less pressure gradient to drive the blood through them), and then stops when the IMP equals the MAP. The IMP usually equals the MAP when the amniotic fluid pressure is around 40 mm Hg. (Remember that the intramyometrial pressure is 2-3 time that of the amniotic fluid pressure). As the contraction eases up, blood flow through the spiral arteries resumes and by the end of the contraction, blood flow is back to normal.
Thus, with each contraction of any significance, there is initially reduced blood flow to the intervillous space, then a cessastion of blood flow, followed by a gradual resumption of blood flow.
On one level, you could imagine the danger of the fetal oxygen supply being interrupted by each uterine contraction. On another level is the realization that for a normal fetus, this interruption is nearly trivial (similar to holding your breath for 5 seconds). But if the contractions are coming too frequently (with very little time between contractions for the fetus to resupply), or if the fetus already has a significant problem, then contractions can pose a threat.
Contraction Patterns
During latent phase labor (prior to 4 cm), contractions may occur every 3-5 minutes and may or may not be painful.
A normal contraction pattern in active labor shows contractions occurring about every 2-3 minutes and lasting about 60 seconds.
If contractions are less often than every 2-3 minutes in the active phase, labor may progress more slowly, if at all. While less frequent contractions are the rule in latent phase labor (prior to 4 cm), they are the exception in active labor.
Coupling
Coupling means that two contractions occur one right after the other rather than the normal pattern. Usually, coupling is followed by a longer contraction-free interval. Tripling can also be seen where three contraction occur without any significant recovery time.
If labor is progressing normally, coupling can be ignored. Often, however, coupling is associated with dysfunctional progress in labor. In these cases, coupling can be treated with:
-
Rest
-
Hydration
-
Narcotics
-
Epidural Anesthesia
- Oxytocin
Tachysystole
If contractions are persistently more often than 5 contractions in 10 minutes, this is called “tachysystole.” Tachysystole poses a problem for the fetus because it allows very little time for resupply of the fetus with oxygen and removal of waste products. For a normal fetus, tachysystole can usually be tolerated for a while, but if it goes on long enough, the fetus can be expected to become increasingly hypoxic and acidotic.
Tachysystole is most often caused by too much oxytocin stimulation. In these cases, the simplest solution is to reduce or stop the oxytocin to achieve a more normal and better tolerated labor pattern. Other causes of tachysystole include:
-
Dehydration
-
Placental abruption
-
Pre-eclampsia
-
Chorioamnionitis
In cases of spontaneous tachysystole, increasing maternal hydration and placement in the lateral decubitus position may slow the contractions.
Periodic Heart Rate Changes
These heart rate changes are recurring throughout labor. They are typically associated in some way with uterine contractions. There are three basic recognized types:
-
Early Decelerations
-
Late Decelerations
-
Variable Decelerations
Each has its own features and clinical significance. In addition, a fetus may demonstrate combined decelerations (for example, a severe variable deceleration with a late deceleration component.)
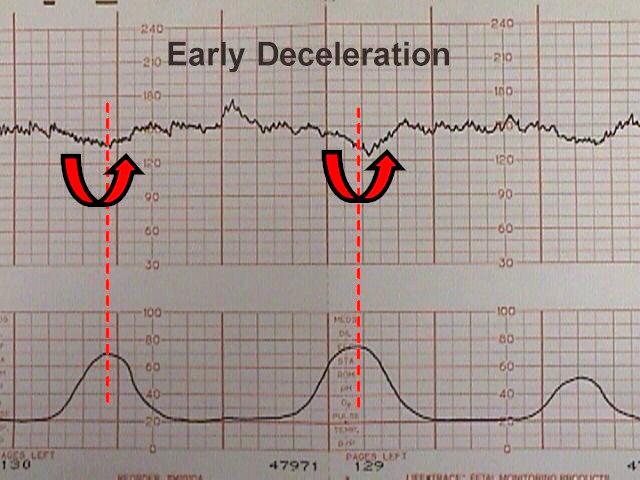  |
Early decelerations are periodic slowing of the fetal heartbeat, synchronized exactly with the contractions. These dips are rarely more than 20 or 30 BPM below the baseline.
These innocent changes are thought to be due, in many cases, to fetal head compression within the birth canal.
Sometimes, patients demonstrating early decelerations will later develop variable decelerations (see below).
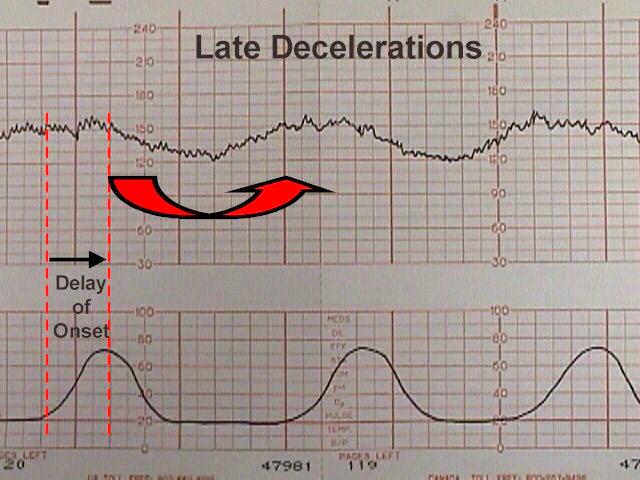
Late decelerations
Late decelerations are repetitive, gradual slowings of the fetal heartbeat toward the end of the contraction cycle. They are felt to represent some degree of utero-placental insufficiency.
All blood flow in and out of the IVS stops briefly during a contraction. A normal fetus with normal reserve (oxygen in its bloodstream, in the blood of the placenta, and in the intravillous space) will probably not notice the tiny drop in total oxygen availability during these contractions. But a fetus who has used up its reserve, or cannot maintain its reserve will, over the course of the contraction, develop some degree of hypoxia, hypercarbia and acidosis. This otherwise normal fetus will respond by slowing its heart rate, to conserve energy. The fetal heart is the largest consumer of oxygen in the fetus and if the rate can be slowed, the fetus will survive longer on less oxygen. After the contraction passes and fresh blood resupplies the intervillous space, the hypoxia, hypercarbia and acidosis is eased and the fetal heart rate returns to normal.
Clinically, the development of late decelerations is a worrisome sign that the fetus has very little reserve. Techniques that may be used to correct this problem include:
-
Changing maternal position to improve uterine blood flow
-
IV hydration to increase maternal blood volume, presumably leading to increased uterine blood flow
-
Administering oxygen to the mother to try to get some additional oxygen through to the fetus. Of the three standard treatments, oxygen administration is the least useful, since the maternal hemoglobin oxygen saturation is likely already 99%. The effect of breathing additional oxygen will probably have minimal effect on the oxygen saturation.
-
Decreasing or discontinuing oxytocin infusion to slow down or stop contractions that are provoking the decelerations.
-
Tocolytic drugs to slow down or stop contractions that are provoking the decelerations.
If the late decelerations are persistent and non-remediable, this is considered “fetal distress,” “fetal intolerance of labor,” or a “non-reassuring fetal heart rate pattern.” Such patients should be delivered promptly to avoid fetal injury or death. Sometimes cesarean section is required to achieve prompt delivery.
If persistent and not correctable, they represent a threat to fetal well-being.
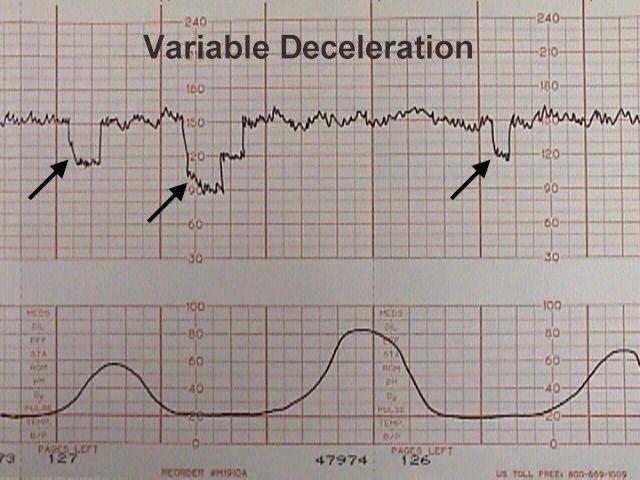  |
Variable decelerations are variable in onset, duration and depth. They may occur with contractions or between contractions.
Typically, they have an abrupt onset and rapid recovery (in contrast to other types of decelerations which gradually slow and gradually recover.
Variable decelerations are thought to represent a vagal response to some degree of umbilical cord compression. If the umbilical cord is only slightly compressed, this will obstruct the umbilical vein (low pressure system) which returns re-oxygenated blood to the fetal heart. The initial normal fetal response to this is a slight increase in fetal heart rate to compensate for the lack of blood return and the slowly diminishing oxygen supplies. If this slight increase in FHR is followed by a major drop in FHR, this phenomenon is called a “shoulder.”
As pressure on the umbilical cord increases, the high-pressure umbilical arteries become occluded. When this happens, there is an immediate rise in fetal blood pressure. 30% of the fetal cardiac output goes to the placenta and if that flow is blocked, the fetus will rapidly develop significant hypertension. The normal fetus will respond to this hypertension by immediately slowing the heart down by sending a signal through the vagus nerve. When the umbilical cord obstruction is released, the vagal response disappears and the fetal heart returns to normal.
If a mild degree of cord compression continues (enough to continue to obstruct the umbilical veins for a while), then another “shoulder” may appear at the end of the deceleration.
If the variable deceleration lasts long enough to cause hypoxia, there may be a more gradual rise back to the baseline and some “overshoot.” Overshoot means the heart rate goes higher than the baseline for a while, to compensate for the mild degree of hypoxia and acidosis that has occurred during that deceleration. If you exercise vigorously for a minute, your muscle tissues will acquire some degree of oxygen debt and a mild degree of local acidosis. When you sit down and rest, your heart rate will be higher than before you started exercising, but will return to normal as you resupply your muscles with oxygen and remove the local waste products. The fetus responds in a similar fashion.
Variable decelerations, unlike late decelerations, are not caused by hypoxia, although if severe enough, frequent enough and persistent enough, can ultimately lead to some degree of fetal acidosis.
The interventions to effectively treat variable decelerations may include:
-
Changing maternal position to improve uterine blood flow
-
IV hydration to increase maternal blood volume, presumably leading to increased uterine blood flow
-
Administering oxygen to the mother to try to get some additional oxygen through to the fetus. Of the three standard treatments, oxygen administration is the least useful, since the maternal hemoglobin oxygen saturation is likely already 99%. The effect of breathing additional oxygen will probably have minimal effect on the oxygen saturation.
-
Amnioinfusion to improve oligohydramnios
-
Decreasing or discontinuing oxytocin infusion to slow down or stop contractions that are provoking the decelerations.
-
Tocolytic drugs to slow down or stop contractions that are provoking the decelerations.
-
Digital elevation of the fetal head out of the maternal pelvis to ease pressure on the umbilical cord.
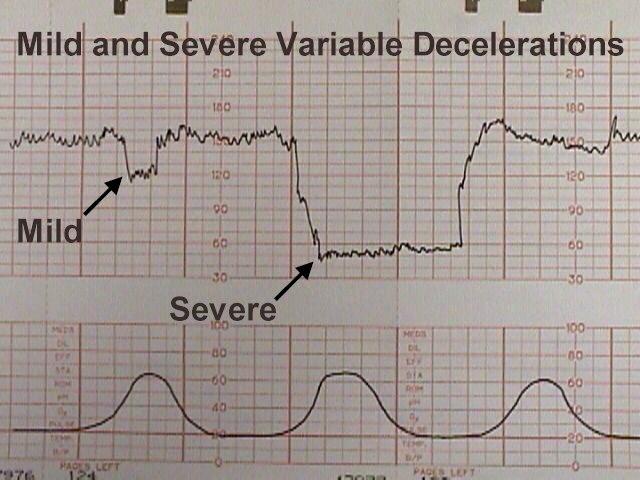
Occasional mild or moderate variable decelerations are common and not considered threatening. They are seen in the majority of laboring patients at some time or other. They are more common in the second stage of labor.
Mild variable decelerations do not dip below 70 BPM and last less than 30 seconds.
Severe variable decelerations dip below 60 BPM for at least 60 seconds (“60 x 60”). If persistent and not correctable by simple means, they can be threatening to fetal well-being. Like persistent, non-remediable late decelerations, fetuses demonstrating persistent, non-remediable severe variable decelerations should be delivered promptly, preferably vaginally, but by cesarean section if necessary.
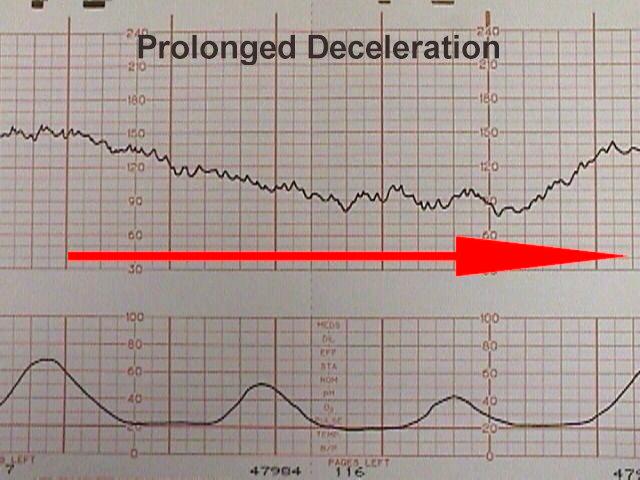 |
Prolonged decelerations
Prolonged decelerations last more than 60 seconds and occur in isolation. Causes include maternal supine hypotension, epidural anesthesia, paracervical block, tetanic contractions, and umbilical cord prolapse.
Some of these are largely self-correcting, such as the deceleration following paracervical block, while others (maternal supine hypotension) respond to simple measures such as repositioning.
Other causes (such as umbilical cord prolapse) require prompt intervention to avoid or reduce the risk of fetal injury.