
LESSON OBJECTIVES
7-1. Select from a list of facts, those facts, which define, team nursing.
7-2. Identify factors related to team productivity.
7-3. Select from a list of facts, those facts that describe a manager and leader.
7-4. Select from a list of personal qualities, those that are qualities of a leader.
7-5. Identify the responsibilities of a team leader.
7-6. Identify five general facts related to patient teaching.
7-7. Identify five steps used in the teaching-learning process.
7-8. Identify factors, which affect patient learning.
7-9. Select from a list of principles, those principles of effective teaching and learning.
7-10. Identify the three types of learning.
7-11. Select from a list, the major type(s) of learning related to a specific teaching strategy.
7-12. Select from a list of guidelines, those guidelines that can help the nurse in ordering the learning experience.
7-1. INTRODUCTION
a. The practical nurses’ role has expanded to team leadership and patient teaching. Leadership is defined as influencing individuals or groups to take an active part in the process of achieving agreed-upon goals. Nursing leadership may be defined as a process of interpersonal influence through which a patient is assisted in the establishment and achievement of goals toward improved well-being.
b. Teaching refers to activities by which specific objectives or desired behavior changes are achieved. It is an interactive process between the teacher and one or more learners. Patient teaching is inherent to the role of nursing by virtue of the nurse’s position at the bedside. Shorter hospital stays which require patients to manage convalescence at home, and emphasis on health promotion and health maintenance rather than on treatment alone, have increased the need for health teaching by nurses.
Section I. TEAM LEADERSHIP
7-2. TEAM NURSING
a. In 1953, Eleanor Lambertson and her colleagues proposed a system of team nursing to overcome the fragmentation of care resulting from the task-oriented functional approach. Team nursing responds to the needs of both the patient and the staff. Team members are stimulated by the team leader to learn and develop new skills. The team leader instructs the team members, supervises them, and provides assignments that offer them potential for growth. The following facts define team nursing:
(1) It is direct patient care accomplished by a specific group of nurses and allied health care workers.
(2) It is accomplished by using the nursing process.
(3) It allows for comprehensive, holistic nursing care when the team functions at a high level of efficiency.
(4) It is composed of a team leader who coordinates patient care and supervises team members, and team members who are responsible for total care given to an assigned group or number of patients.
(5) It requires cooperation and effective communication with all staff members.
b. Basic to team nursing are the team conference, nursing care plan, and leadership skills.
(1) The conference is led by the team leader, and all personnel assigned to the team should be included. The team leader should discuss the needs of the patients, establish goals, individualize the plan of care for each patient, instruct the team members, and follow up on all directions previously given to the team.
(2) The nursing care plan is a written guide that organizes information about a patient’s health. It focuses on the actions that must be taken to address the patient’s identified nursing diagnoses and meet the stated goals. It provides for continuity of care by a constantly changing nursing staff. The team leader starts the care plan as soon as the patient is admitted to the medical treatment facility. In response to changes in the patient’s condition, and evaluation of goal achievement, the nursing care plan is updated and revised throughout the patient’s hospital stay.
(3) Three leadership styles have been described: autocratic, democratic, and laissez-faire. The three are sometimes blended to fit the situation, the needs of the team leader, and/or the needs of the nursing team.
(a) Autocratic leadership. The leader determines policies and gives orders and directions to the members. Autocratic leadership often makes team members dissatisfied. It may be a necessary style when urgent decision-making is required.
(b) Democratic leadership. The leader encourages team discussion and decision-making. This supportive style increases team productivity and satisfaction. Democratic leadership has positive connotations but requires time for discussion. It may not always be the most effective method when team members lack the skills to make decisions or when urgent decision-making is required.
(c) Laissez-faire leadership. The leader participates minimally and acts as a resource person and consultant at the request of the team members. Laissez-faire leadership is described as a “hands-off” approach. It is most effective after the team has made a decision, is committed to that decision, and has the expertise to implement it.
7-3. FACTORS AFFECTING TEAM PRODUCTIVITY
a. Productivity implies effectiveness and efficiency in individual and group performance. To be effective, the objectives must be achieved. To be efficient, the objectives must be achieved with the least amount of resources. Productivity implies measurement. Productivity involves the relative use of skills and the relative use of knowledge. Measurement of skills work is easy, but it becomes more difficult to measure knowledge work. The 91B10 may take and record vital signs of 20 patients in one hour. The team leader may use eight hours completing next month’s schedule, while directing subordinates. One difficulty in measuring the productivity of knowledge work is that often the output contributes indirectly to achieve end results. Factors affecting the nursing team’s productivity are:
(1) The number of team members. A team that is too large wastes time and fosters indecision. The team should be large enough to complete the assigned tasks, but small enough for adequate communication among its members.
(2) The number of assignments. Whatever the situation, the team members must learn to organize their work so that they are able to give adequate care to all of their patients.
(3) The types of tasks to be accomplished. Team members should be competent in performing all tasks that may be assigned. Non-nursing tasks such as answering the telephone, emptying the garbage, and transporting non-acute patients should be eliminated from their duties.
(4) The time allocated to complete the tasks. As conservation of scarce resources such as time, money, and supplies is more vigorously enforced, the need for nurses to be “faster and smarter” in delivering patient care will increase.
(5) The environment. A smaller staff will be on duty during the evening and night. There will be fewer members to a team, and each member will be assigned to care for more patients. Although more personnel are available during the day shift, more patient services are provided. Continuity of care is the key; communication between shifts is vital.
(6) The management style of the team leader. Whether the team leader has an autocratic, democratic, or laissez-faire management style, he must have a thorough knowledge of nursing and an intuitive understanding of human behavior if the team is to produce efficiently.
(7) The skills and experience of each team member. Each team member should have the needed skills for the technique, treatment, or procedure they are to perform. If in doubt, they should know where to find the SOP (standing operating procedures) if required.
b. Although the terms management and leadership are sometimes treated as synonyms, there is a distinct difference between a manager and a leader. The key functions of a manager are planning, organizing, staffing, leading, and controlling. Leadership is an important aspect of managing; however, there can be leaders of completely unorganized groups.
(1) A manager plans and sets up the organizational structure and assigns specific people to accomplish specific tasks.
(2) A leader influences people to be enthusiastic and willing to achieve the desired goals. Leadership and motivation are closely connected.
(3) Team leadership requires some management skills as well as leadership skills.
7-4. LEADERSHIP QUALITIES
a. Although many great nursing leaders emerged in the past, most nurses were kept in subordinate positions. This subordination has diminished as more nurses learn to apply their leadership skills to attain the ultimate goal of improved patient care. Nurses with leadership skills can effect desired changes in the patient’s health patterns, in the medical treatment facility, in the nursing profession, and in the community.
b. Many adjectives are used to describe the traits or qualities of a leader. With education, training, and practice, every nurse can develop the following leadership qualities.
(1) Professional knowledge. Nursing involves knowledge in biology, nursing science, social science, and many other areas. It is impossible to master them all. Learn how to find and use appropriate reference materials and resource persons quickly and efficiently. Keep up with current nursing practices for validity, reliability, and applicability and share your knowledge with peers and subordinates. Political awareness is also required. Know how local, state, and national level legislation will affect health care before supporting candidates or voting. Good leaders must be advocates of patient’s rights in order to improve patient care.
(2) A positive self-image. Leaders must be enthusiastic, dynamic, and self-directed. They must be comfortable with themselves and act as role models to followers.
(3) Effective communication. Leaders must communicate effectively in order to relate to others. The ability to communicate effectively is especially needed when relating to patients, peers, subordinates, and superiors. Effective communication skills are used to:
(a) Share information with team members and involve them in the decision-making process.
(b) Define specific expectations.
(c) Offer suggestions and assistance in the completion of tasks.
(d) Elicit feedback from team members and provide feedback to superiors.
(e) Give constructive criticism and offer positive reinforcement to subordinates.
(f) Practice active listening.
(4) Assertiveness. Leaders need to be assertive in team interaction and other leadership situations. Assertiveness is used extensively when effecting change. Many nurses participate in assertiveness training programs so they can strengthen the position of nursing in the health-care system and increase its influence on patient care.
(5) Flexibility. Changes in the needs of patients, families, and the nursing team can occur within minutes. The nursing role and all nursing functions require flexibility.
(6) An understanding of human needs. The highest level on Maslow’s hierarchy of needs is self-actualization, which is the need for an individual to reach his or her potential through full development of their unique capabilities. Effective leaders seek ways to promote self-actualization in themselves and team members. An effective leader understands the human need to feel useful and important, and the desire to belong, and to be recognized as an individual.
7-5. TEAM LEADER RESPONSIBILITIES
a. The National Federation of Licensed Practical Nurses (NFLPN) Revised Statement of Functions and Qualifications of the Licensed Practical Nurse states that the licensed practical nurse, with additional preparation in specialized areas and under direction of autonomous health professionals, is qualified to:
(1) Supervise other nursing and health-related personnel.
(2) Coordinate and make assignments of other nursing and health-related personnel and patients.
(3) Serve as team leader.
(4) Serve as charge nurse.
b. All members on a nursing team work together under the direction of the physician to help the patient return to his optimum function as quickly as possible. The team leader’s responsibilities are:
(1) To attend change of shift reports. The change of shift report may be given to the entire oncoming shift in one area or it may be given in “walking rounds.” In walking rounds, the departing nurse moves from patient to patient as he or she gives the report to the oncoming staff. This enables the oncoming staff to view the patient’s equipment and dressings as the departing nurse reports what has occurred during her shift.
(2) To assign personnel. Personnel assignments are made with the patient’s needs and each team member’s proficiency in mind. The team leader reviews the nursing care plan, provides each team member with a written assignment sheet, and discusses the assignment with each member. The team leader also assigns breaks and lunch time.
(3) To assist team members with patient care. The team leader may assist with patient care as needed, but usually supervises the care that team members provide and sees that the goals of patient care are being met. He explains procedures to team members.
(4) To coordinate staff activities. The team leader coordinates staff activities to ensure quality patient care. The team leader attends patient care conferences and provides input to the Nursing Care Plan. He keeps abreast of any changes in patient status. He ensures utilization of quality assurance and infection control policies.
(5) To motivate the team. The team leader motivates the team to give skilled nursing care. Self-esteem, status, affiliation with others, affection, giving, accomplishment, and self-assertion are regarded as secondary needs. These needs vary in intensity with various individuals. The team leader must do or say those things, which will influence the team members to act in the desired manner (give skilled nursing care).
(6) To make final rounds. About one hour before the shift ends, the team leader should begin final rounds to observe and assess patient care and patient needs, and to see that everything is in order before the staff goes off duty for that shift. In making final rounds, the team leader would include the following:
(a) Check for completion of assignments.
(b) Check input/output (I&O) sheets.
(c) Check intravenous (IV) infusions and nasogastric (NG) intubations.
(d) Review nursing documentation.
(e) Talk to the patients. Gather information for the change of shift report. Listen for compliments or complaints concerning nursing care.
(f) Thank team members and give constructive feedback to those team members who were unable to complete their assignments.
(7) To complete nursing care rounds. The team leader should visually assess individual patients following the change of shift report.
Section II. PATIENT TEACHING
7-6. FACTS RELATED TO PATIENT TEACHING
a. Patient teaching is a function of nursing and a legal requirement of nursing personnel. Teaching is considered a function of nursing. In some states teaching is included in the legal definition of nursing, making it a required function of nursing personnel by law.
b. Patient teaching is defined as a system of activities intended to produce learning. These activities should help the patient meet individual learning objectives. If they do not, the patient’s need should be reassessed and the activities replaced by others. For example, explanation alone may not teach a diabetic patient how to prepare the syringe for an injection. Actually preparing the syringe may be more effective.
c. Patient teaching is a dynamic interaction between the nurse (teacher) and the patient (learner). Both the teacher and the learner communicate information, emotions, perceptions, and attitudes to the other.
d. Before learning can occur, a relationship of trust and respect must exist between the teacher and learner. The learner trusts the teacher to have the required knowledge and skills to teach and the teacher respects the learner’s ability to reach the goals. This relationship is enhanced by communication that is continuous and reciprocal, once mutual trust and respect have been established.
e. The goal of patient teaching is the patient’s active participation in health care and his compliance with instructions. Once the nurse begins instructing a patient (or family/support persons), the teaching process should continue until the participants reach the goals, change the goals, or decide that the goals will not help meet the learning objectives.
7-7. STEPS IN THE TEACHING-LEARNING PROCESS
a. Assess the Patient’s Learning Needs.
(1) Use all appropriate sources of information. Review the patient’s medical records. Read the history of medical problems as well as diagnoses, physical examinations, documentation of the nursing assessment, and the nursing interventions that have been performed. The patient and the family or support persons are the best source of needs assessment information.
(2) Identify the knowledge, attitude, or skills needed by the patient or family/support persons. Learning can be divided into three domains: cognitive, affective, and psychomotor. You may categorize learning that is planned for the patient into these three areas.
(a) Cognitive involves the storing and recalling of new knowledge and information.
(b) Affective learning includes changes in attitudes, values, and feelings.
(c) Psychomotor learning has occurred when a physical skill has been acquired.
(3) Assess emotional and experiential readiness to learn. Readiness is not the patient’s physical ability to learn. The readiness to learn in an adult may be related to a social role. Being assured that they are partners in the teaching-learning process gives adult learners the sense of control that they are accustomed to in their daily living.
(4) Assess the patient’s ability to learn. The teaching approach must be appropriate to the developmental stage of the learner. You should assess the patient’s intellectual development, motor development, psychosocial development, and emotional maturity. Chronological age does not guarantee maturity.
(5) Identify the patient’s strengths. Learning strengths are the patient’s personal resources such as psychomotor skills, above-average comprehension, reasoning, memory, or successful learning in the past. For example, if the patient knows how to cook, this knowledge can be useful when learning about a special diet.
(6) Use anticipatory guidance. Anticipatory guidance focuses on psychologically preparing a person for an unfamiliar or painful event. When patients know what to expect, anxiety is reduced and they are able to cope more effectively.
b. Diagnose the Learning Needs. Be realistic. When a lack of knowledge, attitude, or skill hinders a patient’s self-promotion of health, the nurse diagnoses the deficit. Confirm your diagnosis with the family. In addition, assess your own knowledge base and teaching skills. You teach information and skills to patients which you lack.
c. Develop a Teaching Plan. Planning ensures the most efficient use of your time and increases the patient’s chances for learning. A teaching plan follows the steps of the nursing process.
(1) Develop measurable learner objectives for each diagnosis of a learning need.
(a) Identify short-term and long-term objectives.
(b) Prioritize the objectives.
(c) Determine who should be included in the teacher-learning process (family members, friends, or other support persons). For example, the person who cooks for the patient is asked to participate in any nutritional teaching.
(d) Include the patient in planning. Ask his permission to involve family members or others.
(2) Create a teaching plan. One nurse or several nurses can prepare and use a teaching plan. There are standardized teaching plans available for major topics of health teaching (some for computer use). Individualize the standardized plans to the patient’s needs and abilities.
(a) Match content with the appropriate teaching strategies and learner activities. For example, content explaining why certain treatments and medications are needed may be matched with printed or audiovisual materials. Children respond well to teaching strategies that permit them to participate actively.
(b) Schedule teaching within the limits of time constraints. Shorter, more frequent sessions allow the patient to digest the new information and prevents him from becoming tired or uncomfortable due to his illness.
(c) Decide on group or individual teaching and formal or informal teaching. Some learner objectives are met more readily in a one-to-one encounter (i.e., colostomy care) while others are met more easily in a group discussion with other patients that have similar problems. Formal teaching is the planned teaching done to fulfill learner objectives. Informal teaching occurs during nursing interactions with the patient and his family. Informal teaching often leads to planned, formal sessions.
(d) Formulate a verbal or written contract with the patient. The contract is informal and is not legally binding; however, such an agreement serves to motivate both the patient and the nurse to attain the learning objectives. It points out the responsibilities of both the nurse (teacher) and the patient (learner). Whether verbal or written, the contract should not be intimidating, but viewed as an aid to learning. Failure to meet contracted objectives should be redirected into new learning and decision-making situations.
d. Implement the Teaching Plan. The implementation phase may be only a few minutes or the sessions may extend over a period of days, or perhaps months. Use interpersonal skills as well as effective communication techniques. Do not use technical and medical terms unless the patient has a medical background, but avoid a condescending attitude. Your attitude has a greater effect on the patient than any other factor. If the patient must learn special techniques or procedures, tell him or her that it takes time and practice to perform these new skills confidently. Review the contractual agreement before implementing the teaching plan.
(1) Prepare the physical environment. It should be a nonthreatening atmosphere, free of distractions and interruptions. Ensure adequate space and lighting, comfortable chairs, good ventilation, and privacy.
(2) Gather all teaching aids: posters, printed material, audiovisual material, and equipment if needed.
(3) Deliver content in an organized manner using planned teaching strategies. If you are teaching a skill or procedure, follow the correct sequence so that the patient is not confused.
(4) Be flexible. Observe the patient for clues or additional assessment data that could alter the original teaching plan. Adapt or reorganize the teaching plan if necessary.
e. Evaluate the Teaching-Learning. Do not assume that learning has occurred without feedback. The key is to write measurable learner objectives in the teaching plan that describe the desired behavior.
(1) Evaluate whether learner objectives have been met. There are several ways to do this.
(a) Observation. Observe the patient to verify that he has put the information that he learned into practice.
(b) Patient’s comments. The patient will usually state whether or not he or she understands the information being taught.
(c) Direct questions. Ask the patient a question requiring a response, which reflects his or her level of knowledge about the topic.
(d) Return demonstration. Have the patient perform the procedure as it was demonstrated. This is an excellent method of evaluating proficiency in psychomotor skills.
(2) Evaluate teaching. Immediately after each session, evaluate your teaching effectiveness.
(a) Quickly review how implementation of the plan went and mentally make note of both your strengths and weaknesses.
(b) Seek feedback from the patients. Use a simple questionnaire with space for comments but one, which requires only check marks to answer. The questionnaires may be more honest and helpful if anonymous.
(3) Revise the teaching plan. Evaluation may reveal that the teaching plan should be revised. Revision is part of the teaching-learning process; it is not an indication of failure. Make adjustments accordingly to meet the patient’s needs.
(a) Alter the content and teaching strategies if the objectives were unrealistic, the content too complex, or the teaching strategy inappropriate.
(b) Employ motivational counseling if the patient is unwilling to participate in learning activities or to learn how to care for himself.
(c) Reschedule teaching sessions if the time and frequency of sessions affected the teacher-learner process.
(4) Document the teaching-learning process. Teaching is an important and required nursing responsibility; it must be documented in the patient’s record.
(a) Include a summary of the diagnosed learning needs, the teaching plan, implementation of the plan, and evaluation results.
(b) Show evidence in the evaluation statement that learning has occurred, or how the problem was resolved if the patient or support person did not learn the material taught.
7-8. FACTORS WHICH AFFECT LEARNING
a. Factors, which affect patient learning, need to be assessed in order for appropriate teaching strategies to be used.
b. Include the following factors in your assessment.
(1) Developmental considerations. Knowledge of intellectual, psychosocial, and physiologic age is necessary before you select age-appropriate teaching methods. Delayed development in any of these areas should be considered.
(a) Children have limited past experiences. Adults learn more quickly than children because they are able to build upon previous knowledge.
(b) Use chronological age to assess whether the developmental stage is as would be expected.
(2) Educational level. You will effectively promote learning if you are aware of the learner’s intellectual ability and avoid “talking down” to him or her or using an inappropriate teaching strategy.
(3) Past learning experiences. Attitudes toward future learning are influenced by learning experiences in the past. Encourage the learner to express how he views education so that you can deal with his feelings before teaching is attempted.
(4) Physical condition. The patient will not be ready to learn until he is comfortable enough to pay attention to the information you present.
(5) Sensory abilities. Note any deficit in the learner’s sight, hearing, and touch so that teaching is planned appropriately.
(6) Emotional health. The emotional state of the learner should be conducive to learning before teaching is done.
(a) A patient, who is moderately anxious about his/her condition, will probably be attentive to presentation of information that will help him manage the condition.
(b) If the patient is in a state of crisis with a high level of anxiety, delay teaching until the crisis is over.
(7) Social and economic stability. Being hospitalized and absent from work cause some patients excessive stress. Help the patient deal with any social and economic problems before imposing the additional stress of learning information or a new skill.
(8) Responsibility. To learn self-care or take preventive measures against illness, a patient must have a sense of responsibility. Encourage the patient to participate in planning the learning activities to promote his feelings of control.
(9) Self perception. Self-perception has an effect on the ability to learn. If effective learning about a health problem is to occur, any unrealistic self-image or body image should be addressed. If necessary, help the patient improve self-image before focusing on learning needs.
(10) Attitude toward learning. Attitude toward learning is difficult to measure. Talk to the patient to get an idea of how he feels about learning to improve his health. If the patient has a negative attitude about learning, establish a relationship that will help in altering that attitude.
(11) Motivation to learn. The patient must want to learn for teaching to be effective. If the patient is not motivated to learn the material needed to improve his health, discussing his interest and concerns may lead to success.
(12) Culture. Some cultures value education that will improve their condition, while others view change or new practices as threatening. Do not stereotype any person because of his culture; but recognize that each person has a unique family background with certain cultural values that may have an effect on how teaching learning is perceived.
(13) Communication skills. The basic requirement for the teaching-learning process is communication. Assess your communication skills as well as those of the learner.
(a) Assess the learner’s reading skills before using printed material as a teaching aid.
(b) Assess to what degree English is spoken and understood by the learner. Most hospitals have printed and audiovisual materials available for non-English speaking patients.
7-9. PRINCIPLES FOR EFFECTIVE TEACHING-LEARNING
a. These basic principles are effective guidelines when applied in situations in which the teaching-learning process is used by nurses to meet the needs of clients.
NOTE: Clients may be patients, family members, or support persons.
(1) The teaching-learning process is facilitated by the existence of a helping relationship.
(a) A helping relationship exist among people who provide and receive assistance in meeting a common goal. The relationship is established as a result of communication.
(b) The communication is continuous and reciprocal.
(2) Nurses in the role of teachers must be able to communicate effectively with individuals, with small groups, and in some instances with large groups.
(3) Knowledge of the communication process is necessary for the assessment of verbal and nonverbal feedback.
(4) A thorough assessment of clients and the factors affecting learning helps to diagnose their learning needs accurately.
(5) The teaching-learning process is more effective when the client is included in the planning of learner objectives.
(6) Unless the client values these objectives, little learning is likely to occur.
(7) The implementation of a teaching plan should include varied strategies for sensory stimulation, which apparently promote learning.
(8) Relating new learning material to clients’ past life experiences is effective in helping to assimilate new knowledge.
(9) Proposed behavioral changes must always be realistic and explored in the context of the client’s resources and everyday life-style.
(10) Careful attention should be paid to time constraints, scheduling, and the physical environment.
(11) Learner objectives provide the basis for evaluating whether learning has occurred.
(12) When learning objectives have not been met, careful reassessment provides ideas for changing the teaching plan for subsequent implementation.
b. The teaching-learning process and the nursing process are interdependent. Patient teaching is approached more effectively if the steps of the nursing process are followed.
7-10. TYPES OF LEARNING
a. Three domains, or types of learning, have been identified as cognitive, affective, and psychomotor.
(1) The cognitive domain includes intellectual skills such as thinking, knowing, and understanding. When the patient stores and recalls information, he is using the cognitive domain. For example, after attending classes on the low sodium diet a patient states how salt affects the blood pressure.
(2) The affective domain includes feelings, emotions, interests, attitudes, and appreciations. An example would be a patient’s acceptance of having a colostomy and maintaining his self-esteem.
(3) The psychomotor domain involves motor skills. An example would be a patient demonstrating clean technique when changing her dressing.
b. Nurses should include each of these three domains in patient teaching plans (see paragraph 7-7a(2)).
7-11. SELECTING TEACHING STRATEGIES
a. Consider the different teaching strategies during the planning stage and choose a method of teaching that is suited to the individual being taught, for the material to be learned, and for you, the teacher.
b. Consider the content and the types of learning. The content to be taught is determined by the objectives. For example, when teaching self-care to a recently diagnosed diabetic, one of the objectives may be “Identify appropriate sites for insulin injections.” This means that you must include content about body sites suitable for insulin injections. You should have some knowledge of sources for content information as a result of your own education and training.
c. Consider the following in matching sources of content information with a suitable strategy for the individual learner and for you, the nurse-teacher:
(1) A person who cannot read needs a source of content material in other than printed form. Use of games and role-play are popular and fun ways for children to learn.
(2) Discussion is not the best strategy for teaching a psychomotor skill. Demonstration of techniques using a practice model is an effective way of teaching someone to give an injection.
(3) Some people are visually oriented and learn best through seeing. Others learn best through hearing; an explanation or one-on-one discussion may be the most suited method.
(4) The nurse-teacher must be a competent group leader to use group discussion as a teaching strategy.
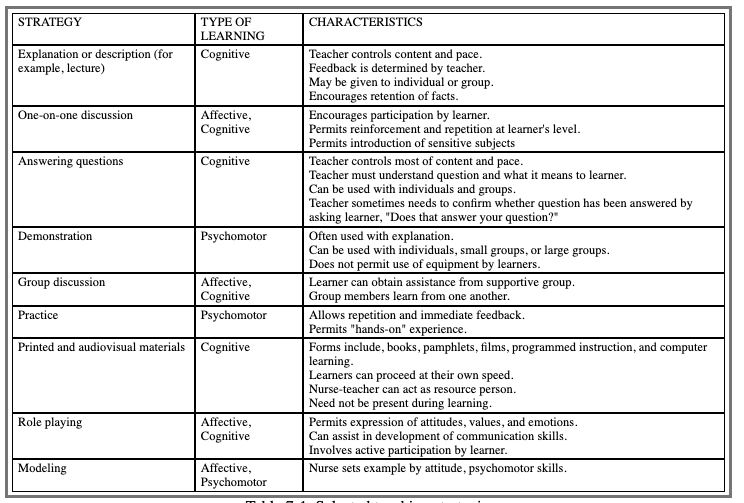
d. Some methods are better suited to certain learning objectives than others. A 10-year old recovering from burns as a result of playing with matches would be receptive to a comic book on personal safety; an adult burn victim could learn similar information by discussing safety measures. Use of a variety of teaching strategies aids learning. See Table 7-1 for selected teaching strategies for the three types of learning and characteristics of each strategy.
7-12. SEQUENCING THE LEARNING EXPERIENCES
a. Whether formal or informal, teaching requires a plan or it becomes haphazard and the patient’s need for information goes unattended. The following guidelines are helpful in sequencing or ordering the learning experiences.
(1) Learning is facilitated when there is some personal interest. Start with something the learner has identified as a need or concern. For example, before he learns how to administer insulin to himself, an adolescent is seeking information on adjusting his lifestyle so that he can still play football.
(2) Start with what the learner knows and proceed to the unknown. If you do not know the patient’s knowledge or skill level, illicit this information by asking questions or having the patient complete a form.
(3) Teach an area that is anxiety provoking first, if the learner has a high level of anxiety that can impair concentration in other areas. For example, women cannot concentrate on learning to bathe her husband in bed because she is highly anxious about being able to move him and turn him in bed.
(4) Teach the basic concepts first when there are variations or adjustments in a procedure, then proceed to the variations or adjustments. Learners may become confused if they have to consider variations and adjustments before understanding the basic concepts of a procedure. For example, teach a patient how to insert a Foley catheter before teaching him what to do if the catheter stops draining.
7-13. CLOSING
The role of the practical nurse varies with the situation. Practical nurses actively participate as team leaders, managers, and teachers. The traditional skills of nurses were psychomotor skills involving use of the hands. Individualizing care and communicating activities require nurses to use affective skills. Cognitive skills are required in all aspects of the nursing process. These expanded nursing roles have established new dimensions for nursing practice.