
Introduction to the Operating Room
LESSON 1: ORIENTATION
1-6
1-6. PHYSICAL LAYOUT
a. Arrangement. Basic principles for efficient workflow are adhered to when planning the arrangement of rooms within a surgical suite. For example, traffic must move smoothly and without interruption into, through, and out of the suite. Those rooms where support activities are performed are grouped conveniently and systematically about the ORs, which are arranged in pairs with scrub rooms and sterilizing facilities between them. (See figure 1-3). Proper arrangement of the rooms reduces the flow of excess traffic, saves much unnecessary walking, and therefore conserves time and effort.
b. Size of the Suite. Numerous factors are considered when estimating the size of the surgical suite required for a hospital.
(1) The first of these is the operative load or the number of surgical cases to be done per day. Some hospitals have more patients requiring medical care than surgical care. In such a hospital, only a small operative section would be necessary. Several operative procedures can be done per day in each OR, one case following another, but all should be completed by the end of the usual day shift or shortly thereafter.
(a) The average number of ORs needed is indicated by the number of operative cases to be done daily divided by the number of cases that can be done daily in one OR.
(b) Operative load can also be broadly interpreted to include the amount of work to be done per day, outside of actual cases. There is a great deal of preparatory work necessary for each surgical procedure as well as the routine tasks to maintain the suite. If most supplies are prepared and sterilized in CMS, the OR suite needs to maintain only a small preparation and sterilization area; otherwise, it may need a large one.
(2) The second factor, the types of surgery to be done, is even more specific. Some procedures such as cardiac surgery are very long and detailed, requiring many hours of operative time; others, such as tonsillectomy, can be accomplished in just 20 to 30 minutes. In the first instance, a single OR would be engaged for the whole operative day with just one case; in the second example, eight or ten such procedures could be done in the same length of time.
(3) The number and frequency of emergency cases are also considerations related to the necessary size of the suite. The larger the troop area near a hospital, the greater the number of accident and emergency cases that may have to be done. These must be done immediately, meaning that other scheduled cases may have to wait until after normal duty hours, unless provision has been made for an additional room.
c. Size of Individual Operating Room. In addition to plans for the number of ORs required, the size of each room must also be considered. Certain types of surgery require the use of much bulky equipment. This is especially true of open-heart surgery, during which large machines are required to pump and oxygenate the blood outside of the body and to monitor the functioning of the heart. Factors such as this must be planned for and sufficient floor space provided so that breaks in aseptic technique due to overcrowding will be avoided. On the other hand, rooms should be no larger than necessary, thus reducing the amount of unnecessary times spent walking. The Army criteria for square footage per room are sufficiently flexible to provide for the needs of its hospitals. (See figure 1-3, "Type" floor plan for an Army hospital-operating suite.)
d. Four Areas. The designations listed in the Four Zone Concept (1) thru (4) are not necessarily used for all hospitals, but whenever feasible the surgical suite is segregated into four areas for traffic control. The purpose of such control is to assure maximum protection against infections. In analyzing the traffic and commerce system of the OR system, specific traffic patterns must be determined. These are dependent on the entrances and exits for both personnel and materials. Renovation planning of existing facilities should consider renovation of central supply and storage areas to bring these as close to the point of utilization as possible. Where entirely new wings, buildings, or entire hospital complexes are being considered, there is opportunity to design traffic, materials-handling, and storage systems around the requirements of the surgical suite. Traffic control design is aided by designation of the four-zone concept (as shown below): the interchange area, semirestricted area, restricted area, and dirty area.
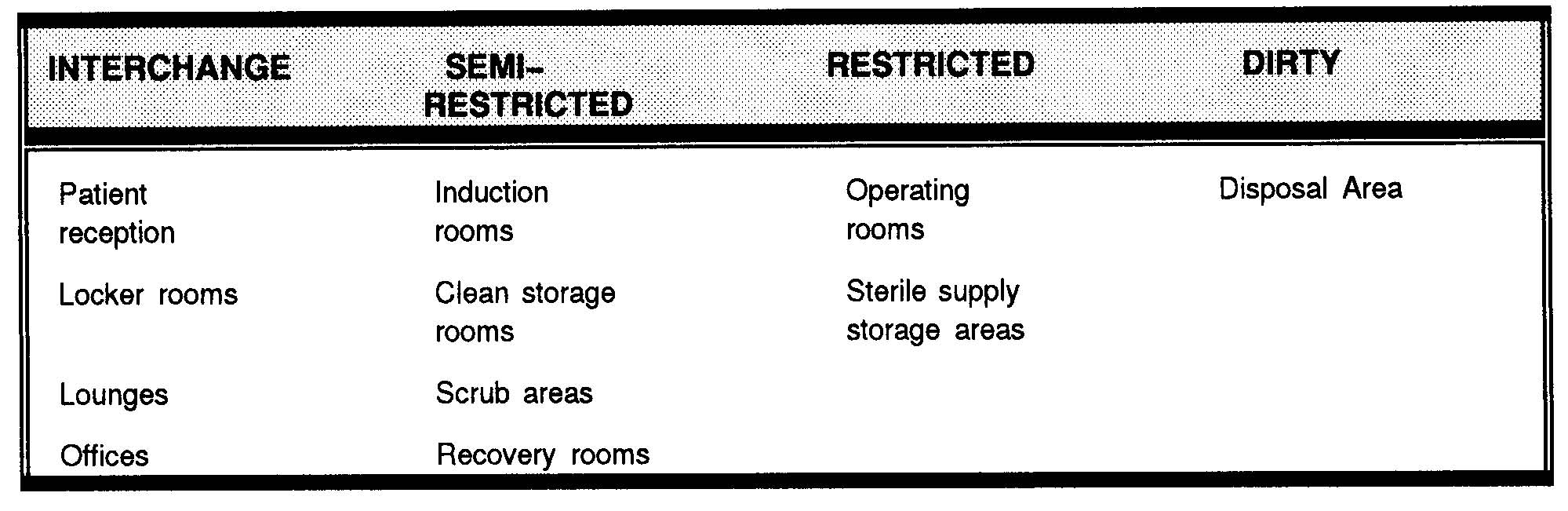
Four-zone concept.
(1) Interchange area. The interchange area is provided to enable persons from outside the surgical suite to meet with personnel within the suite when necessary. Examples of such rooms are the offices--one for the OR supervisor and one for the chief of anesthesiology (see figure 1-3 (18) and (19))--whenever the offices for these personnel are situated within the surgical suite. In some hospitals, these offices are located convenient to but outside the surgical suite in order to keep traffic within the suite to a minimum. If there is a postanesthesia (recovery) room, it is also classified as an interchange area although entry is carefully
controlled. The main outer corridors are in the interchange area. This area also consists of the rooms designed for personnel to change from street clothes or military uniforms into OR attire ("scrub clothing") (see figure 1-3 (15), (16), and (17)). If space and arrangement permit, there are two doors to each dressing room--one for the entry of persons in street clothes and the other for their exit in scrub clothes. The individual lockers are generally equipped with nametags, locks, and keys. Caps, masks, and scrub clothing are stored in the dressing rooms. Dressing rooms may be equipped with showers. A mask need not be worn in this area.
(2) Semirestricted area. Comprising the semirestricted area are corridors within the work area, the anesthesia workroom and storage, the utility closet, the instrument storage room, the workroom, the linen storage room, the clean linen room, and the soiled linen room (see figure
1-3 (4), (5), (7), (8), (10), (11), (12), (13), and (14)). The semirestricted area then represents the supply center for the surgical suite. Although, non-sterile procedures are performed in this area, personnel without OR attire are not admitted. A mask need not be worn in this area.
(3) Restricted area. The restricted area consists of all rooms in which sterile procedures are done and sterile goods are opened or exposed. This includes the individual ORs and the adjacent scrub rooms (see figure 1-3) where soap, nail files, brushes, timers, and written directions are available for the scrub procedure. Also included are the preanesthesia rooms (induction rooms) if the suite has this facility. On the floor plan shown in figure 1-3, a part of the "anesthesia area," (4), may be designated for the induction of anesthesia. If the suite is arranged to include a substerilizing room between each two ORs (see figure 1-3 (3)), then these rooms are considered to be restricted because supplies are autoclaved here without being covered and are moved, uncovered, into the OR. Each person working in the restricted area is required to wear scrub clothes, cap, and mask.
(4) Dirty area. The dirty area is the disposal area, where all utilized materials and linen are gathered, packaged, and sent to appropriate areas.
e. Arrangement of Areas. There is no one rule that must be followed in the physical arrangement of the four areas previously discussed. However, the nonrestricted and interchange areas should be located near the entry door. Workroom areas are situated near the center of the suite, and storage and supply rooms nearby are positioned to avoid waste in time and energy of personnel. Areas for storage of both sterile and unsterile supplies must be clearly marked to avoid mistaking one for the other. If there is no linen chute in the suite, a room for soiled linen is necessary (see figures 1-3 (14)). This room is classified as semirestricted. If the suite has observation galleries, these are provided with outside entries to eliminate unnecessary traffic of persons in street clothing.
