
Cardiopulmonary Resuscitation
LESSON 4: PERFORM CARDIOPULMONARY RESUSCITATION ON AN ADULT
4-2
4-2. ADMINISTER CARDIOPULMONARY RESUSCITATION TO AN ADULT USING THE TWO-RESCUER METHOD
If you have another person qualified to administer CPR ready to help you, two-rescuer CPR should be performed. In two-rescuer CPR, one rescuer is responsible for administering chest compressions while the other rescuer is responsible for administering ventilations. In this paragraph, it is assumed that you have already moved the casualty to safety if required (paragraph 3-1), checked for responsiveness (paragraph 3-2), called for help (paragraph 3-3), checked for spinal injury (paragraph 3-4), and positioned the casualty on his back on a firm surface (paragraph 3-5). It is also assumed a soldier who is qualified to perform two-rescuer CPR has answered your call for help.
a. Position Yourselves. One rescuer positions himself at the side of the casualty's head. This rescuer (called the ventilator rescuer from now on) will administer ventilations to the casualty. The other rescuer positions himself at the casualty's chest on the opposite side from the ventilator rescuer (figure 4-4). The second rescuer (called the compressor rescuer from now on) administers the chest compressions. Rescuers should be on opposite sides of the casualty so that each rescuer has room to perform two-rescuer CPR. If both rescuers must be on the same side (in a ground ambulance, for example), both rescuers must be careful to avoid accidental contact which could interfere with the efficiency of their CPR efforts.
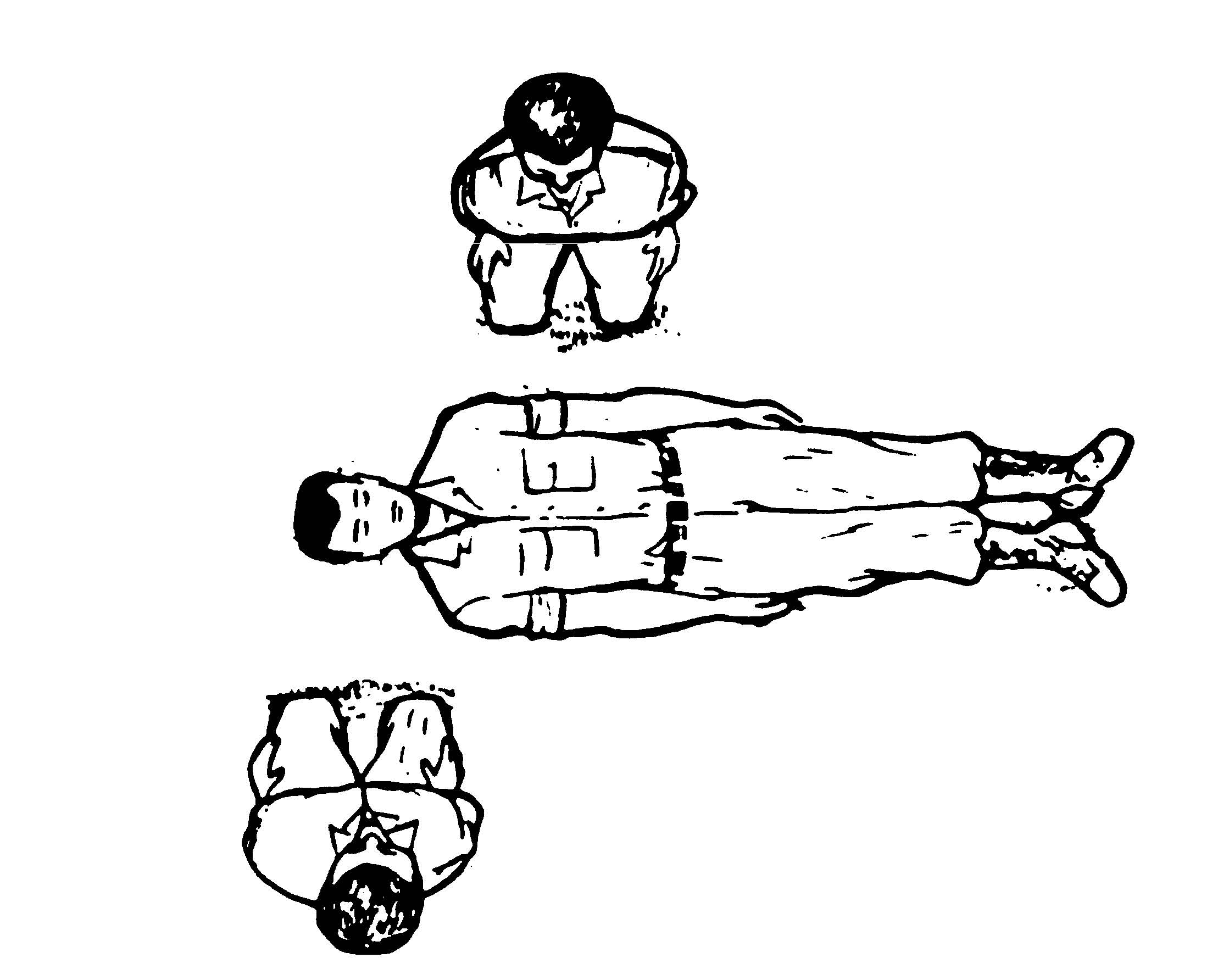
Figure 4-4. Rescuers positioned for two-rescuer CPR.
b. Evaluate Casualty. The ventilator rescuer (the rescuer at the casualty's head):
(1) Opens the casualty's airway (paragraph 3-6).
(2) Checks for signs of breathing (paragraph 3-7).
(3) Administers two full breaths if spontaneous breathing is not present and observes the casualty's chest to make sure that it rises (paragraph 3-9).
(a) If the airway is blocked, the ventilator rescuer opens the casualty's airway more and tries to administer two ventilations again. If the ventilations are unsuccessful, he tells the compressor rescuer to administer thrusts (paragraph 5-6f) while he (ventilator rescuer) performs finger sweeps (paragraphs 5-6c) as needed until the obstruction is removed.
(b) After the obstruction is removed, the ventilator rescuer administers two breaths and two-rescuer CPR is continued.
(4) Checks for a pulse by feeling the carotid artery for 5 to 10 seconds (paragraph 3-11).
(5) Informs the compressor rescuer of the need for chest compressions by saying, "No pulse," if a pulse is not detected.
c. Prepare for Chest Compressions. While the ventilator rescuer is evaluating and ventilating the casualty, the compressor rescuer (the rescuer at the casualty's chest):
(1) Locates the site for administering chest compressions (paragraph 4-1d).
(2) Positions himself to administer the compressions (paragraphs 4-1e and 4-1f).
d. Administer 30 Compressions. When the ventilator rescuer says, "No pulse," the compressor rescuer administers 30 chest compressions at the rate of approximately 100 compressions per minute. The sternum is depressed 1 1/2 to 2 inches with each compression.
(1) The force of the compression should be delivered straight down without rocking the casualty. The fingers should not touch the casualty.
(2) The release part of the compression should be equal in time to the thrust part of the compression. Both parts should be distinct (no bounce).
(3) The compressor rescuer must keep his compressions regular and keep track of compression by counting out loud, "one and two and three and four and five and…." He must also push fast and hard to ensure a fast enough rate of compressions and adequate depth.
(a) The compressor rescuer pushes down on the sternum when he says a number.
(b) The compressor rescuer releases the pressure when he says, "and."
e. Administer Two Breaths. After the compressor rescuer says "thirty," the ventilator rescuer blows two breaths into the casualty's mouth (or nose). This must be done while the chest compression is in the "release" portion. If the ventilator rescuer blows air into the casualty's lungs while the compressor rescuer is performing the "push" portion of a chest compression, the actions would interfere with each other and be inefficient. Each ventilation should take about 1 second.
f. Continue Cardiopulmonary Resuscitation Cycles. After the ventilator rescuer administers the ventilations, the compressor rescuer administers 30 more chest compressions. Although there is a slight break between the last compression of a cycle and the first compression of the next cycle to allow for the ventilation, the compressor rescuer should not remove his hands from the casualty's chest between cycles. While the compressor rescuer is delivering compressions, the ventilator rescuer feels the casualty's pulse to ensure that the compressions are being effective. Both rescuers continue administering two-rescuer CPR cycles until 5 cycles have been administered. Each two-rescuer CPR cycle (sometimes called a 30:2 cycle) consists of thirty chest compressions followed by two full ventilations. At this rate, a casualty will actually receive about 150 compressions and 10 breaths after two minutes.
g. Check for Spontaneous Pulse and Respiration. After the first five cycles (2 minutes), the compressor rescuer stops administering compressions and the ventilator rescuer checks for spontaneous pulse and respiration. The check should take about 5 seconds.
(1) If the casualty has spontaneous heartbeat and respiration, the ventilator rescuer informs the compressor rescuer that the casualty is breathing on his own. The compressor rescuer then checks the casualty for injuries while the ventilator rescuer continues to maintain the casualty's airway and monitor the casualty's respirations and pulse.
(2) If the casualty's heart is beating on its own, but the casualty is not breathing on his own, then the ventilator rescuer informs the compressor rescuer of the situation and begins administering rescue breathing. The compressor rescuer then checks for other injuries. If the casualty's pulse stops again, two-rescuer CPR is resumed.
(3) If no pulse is detected after checking for 5 seconds, the ventilator rescuer opens the casualty's airway, administers two breaths, and says, "No pulse." The compressor rescuer resumes administering chest compressions and two-rescuer CPR is continued.
h. Continue Cardiopulmonary Resuscitation Cycles and Checks. If the pulse is absent, continue to administer two-rescuer CPR using the cycle of thirty chest compressions followed by two breaths. After administering CPR for about two minutes, both rescuers stop their efforts and the ventilator rescuer checks the casualty for spontaneous pulse and breathing. If the check shows no change, two-rescuer CPR is resumed. A check is made every five cycles (about every 2 minutes).
i. Switch When Needed. If the rescuer administering chest compressions becomes tired, the rescuers can switch functions. (Note: The same general procedures can be used if another qualified rescuer appears and wishes to give one of the rescuers a rest.) It is important to change compressors about every two minutes to ensure adequate rate and depth of compressions.
(1) The rescuer administering the chest compressions calls for the switch by counting "CHANGE and two and three and four and five…"
(2) After the compressor rescuer gives the thirtieth chest compression, he moves to the position for giving rescue breathing at the casualty's head without moving to the casualty's other side.
(3) The ventilator rescuer administers two breaths after the thirtieth compression and moves to the casualty's chest without changing sides.
(4) The rescuer at the casualty's head (formerly the compressor rescuer, now the ventilator rescuer) checks for spontaneous heartbeat and breathing (about 5 seconds).
(5) The other rescuer (formerly the ventilator rescuer, now the compressor rescuer) locates the chest compression site and positions himself to deliver chest compressions.
(6) If the casualty still has no pulse, the new ventilator rescuer says, "No pulse," and administers two ventilations. The new compressor then begins administering chest compressions. Both rescuers continue to administer two-rescuer CPR.
(a) If the casualty's heart has resumed beating but the casualty is not breathing, the new ventilator rescuer continues to administer rescue breathing while the other rescuer looks for injuries.
(b) If the casualty has spontaneous pulse and respiration, the new ventilator rescuer maintains the casualty's airway and monitor his respirations and pulse, while the other rescuer checks the casualty for injuries.
j. Evacuate the Casualty. If possible, evacuate the casualty to a medical treatment facility. Continue administering CPR or rescue breathing as needed. If the casualty is breathing on his own, one must monitor his respirations and pulse closely, since his condition could deteriorate rapidly without warning.
k. Terminate Efforts, If Required. Keep administering CPR until one of the following occurs.
(1) The casualty's heart is beating on its own.
(2) You are relieved by another qualified person.
(3) You are ordered to stop by a physician or other authorized person.
(4) You are too exhausted to continue your efforts.
