This is the Archived Desktop Edition.
You should be transferred to the Newest Edition for Desktop and Mobile within 2 seconds.
![]()
Multimedia Edition
Lesson 7: Characteristics of the Typical Newborn Infant
The nurse is in a unique position to aid the newborn infant in the stressful transition from a warm, dark, fluid-filled environment to an outside world filled with light, sound, and novel tactile stimuli. During this period of the newborn adjusting from intrauterine to extrauterine life, the nurse must be knowledgeable about a newborn's normal biopsychosocial adaptations to recognize any deviations. To begin life as an independent being, the baby must immediately establish pulmonary ventilation in conjunction with marked circulatory changes. These radical and rapid changes are crucial to the maintenance of life. All other neonatal body systems change their functions or establish themselves over a longer period of time. The nurse performs an initial assessment to evaluate the neonate, its immediate postbirth adaptations, and the need for further support.
7-2. VITAL SIGNS OF THE NEWBORN INFANT

a. Temperature Regulation.
(1) The infant's body temperature drops immediately after birth in response to the extrauterine environment. His internal organs are poorly insulated and his skin is very thin and does not contain much subcutaneous fat. The infant's heat regulating mechanism has not fully developed. His temperature rapidly reflects that of his environment. The flexed position that the infant assumes is a safeguard against heat loss because it substantially diminishes the amount of body surface exposed.
(2) Nursing implications are centered on regulating an environment to provide constant body temperature of a neutral thermal environment. The infant is placed in blankets, hat, and a controlled temperature environment after birth to counteract the drop in body temperature that occurs immediately after birth. After admission to the nursery, the infant is placed in isolation (isolette) and a temperature probe may be used for continuous monitoring. The infant's axillary temperature is maintained at 36.4 to 37.2o C.
NOTE: An isolette is a self-contained unit that controls the temperature, humidity, and oxygen concentration for an infant.
b. Pulse. The normal pulse range for an infant is 120 to 140 beats per minute (bpm). The rate may rise to 160 bpm when the infant is crying or drop to 100 bpm when the infant is sleeping. The apical pulse is considered the most accurate.
c. Blood Pressure. The average blood pressure (BP) of an infant at birth is 72/42. A drop in systolic BP of about 15 mm Hg the first hour after birth is common. The newborn's BP may be taken with a Doppler blood pressure device. This greatly improves accuracy.
d. Respirations. The respirations of a newborn infant are irregular in depth, rate, and rhythm and vary from 30 to 60 beats per minute. Respirations are affected by the infant's activity (that is, crying). Normally, respirations are gentle, quiet, rapid, and shallow. They are most easily observed by watching abdominal movement because the infant's respirations are accomplished mainly by the diaphragm and abdominal muscles (see figure 7-1). No sound should be audible on inspiration or expiration.

Figure 7-1. Infant's respirations.


7-3. CHARACTERISTICS OF THE NEWBORN INFANT'S HEAD
The newborn infant's head represents one-fourth of his total body length. Its circumference is equal to that of his abdomen or chest. The average size is 13" to 14" (33-35 cm). The head is shaped or molded as it is forced through the birth canal in vertex presentations.
a. Molding. During delivery, for the large head to pass through the small birth canal, the skull bones may actually overlap in a process referred to as molding. Such molding reduces the diameter of the skull temporarily. This elongated look usually disappears a few hours after birth as the bones assume their normal relationships (see figure 7-2).
b. Fontanels. The infant's skull is separated into six bones one from another along the suture lines (see figure 7-3). Where more than two bones come together, the space is called a fontanel. This is the unossified space or soft spot between the cranial bones of the skull in an infant. The infant's pulse is sometimes visible there. The anterior fontanel is located at the intersection of the sutures of the two parietal bones and the frontal bones. It is diamond-shaped and strongly pulsatile. It normally closes at 9 to 18 months of age. The posterior fontanel is located at the junction of the sutures of the 2 parietal bones and 1 occipital bone. It is small, triangular shaped, and less pulsatile. It normally closes at 1 1/2 to 3 months of age. The anterior fontanel is the larger of the two.
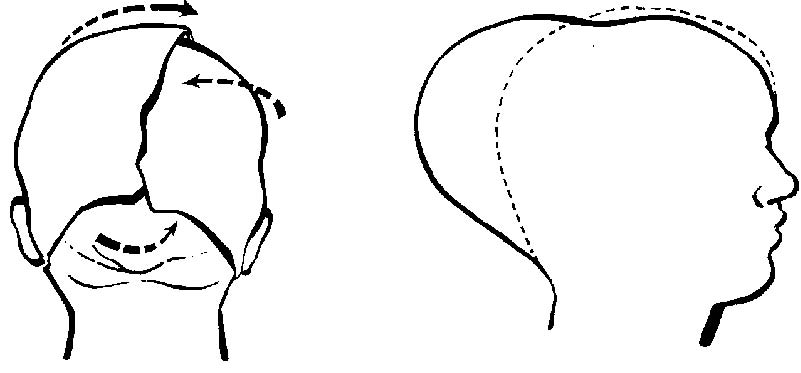
Figure 7-2. Molding of infant's head.

c. Cephalohematoma. This is a collection of blood between a cranial bone and its overlying periosteum (see figure 7-4). Bleeding is limited to the surface of the particular bone. It is caused by pressure of the fetal head against the maternal pelvis during a prolonged or difficult labor. This pressure loosens the periosteum from the underlying bone, therefore rupturing capillaries and causing bleeding. It may be apparent at birth but sometimes are not seen until 24 to 48 hours of life because subperiosteal bleeding is slow. It varies in size, rather firm to the touch and tends to increase in size from 1 to 3 days and then become softer and more fluctuant. Most cephalhematomas are absorbed within several weeks. No treatment is required in the absence of unexplained neurologic abnormalities.
d. Caput Succedaneum. This is an abnormal collection of fluid under the scalp on top of the skull that may or may not cross the suture lines, depending on the size. Pressure on the presenting part of the fetal head against the cervix during labor may cause edema of the scalp (see figure 7-4). This diffuse swelling is temporary and will be absorbed within 2 or 3 days.

Figure 7-4. Cephalohematoma and caput succedaneum.
|

7-4. CHARACTERISTICS OF THE NEWBORN INFANT'S EYES AND EARS
a. Eyes. The infant's eyes may be folded and creased and may seem out of shape because they contain little hardened cartilage. The infant's eyes may not track properly and may cross (strabismus) or twitch (nystagmus). This will cause concern if it extends beyond six months.
(1) Color. At birth, the iris color is usually grayish-blue in Caucasians and grayish brown or brown in dark-complexioned races. A gradual deposition of pigment produces the final eye color of the baby at the age of three to six months and sometimes it may take a year.
(2) Pupils. The pupils do react to light and the infant can focus on objects about eight inches away. The infant's blinking is a natural protection reflex.
(3) Lacrimal apparatus. The lacrimal apparatus is small and nonfunctioning at birth and tears are not usually produced with crying until one to three months of age.
b. Ears. The infant's ears tend to be folded and creased. A line drawn through the inner and outer canthi of the eye should come to the top notch of the ear where it joins the scalp (see figure 7-5). The infant usually responds to sound at birth.

Figure 7-5. Structure of infant's ear.
7-5. CHARACTERISTICS OF THE NEWBORN INFANT'S SKIN



The infant has delicate skin at birth that appears dark red because it is thin and layers of subcutaneous fat have not yet covered the capillary beds. This redness can be seen through heavily pigmented skin and becomes even more flushed when the baby cries.
a. Vernix Caseosa. This is a soft, white, cheesy, yellowish cream on the infant's skin at birth (see figure 7-6). It is caused by the secretions of the sebaceous glands of the skin. It offers protection from the watery environment of the uterus, is absorbed in the skin after birth, and serves as a natural moisturizer. If there is a large amount of vernix caseosa present, it should be meticulously removed as it is thought to be a good culture medium for bacteria.
b. Lanugo. This is a long, soft growth of fine hair on the infant's shoulders, back, and forehead. It disappears early in postnatal life.
c. Mongolian Spots. These are blue-black colorations on the infant's lower back, buttocks, and anterior trunk. They are often seen in infants of Black, Indian, Mongolian, or Mediterranean ancestry. These spots occur less frequently in Caucasian babies. The spots are not bruises nor are they associated with mental retardation. They disappear in early childhood.
d. Jaundice. This is a yellow discoloration that may be seen in the infant's skin or in the scera of the eye. Jaundice is caused by excessive amounts of free bilirubin in the blood and tissue.
e. Petechiae. These are small, blue-red dots on the infant's body caused by breakage of tiny capillaries. They may be seen on the face as a result of pressure exerted on the head during birth. True petechiae does not blanch on pressure.
f. Milia. These are tiny sebaceous retention cysts. They appear as small white or yellow dots and are common on the nose, forehead, and cheeks of the infant. They are of pin head size and opalescent. Milia is due to blocked sweat and oil glands that have not begun to function properly. They disappear spontaneously within a few weeks.
g. Birthmarks.
(1) These are small, reddened areas sometimes present on the infant's eyelids, mid-forehead, and nape of the neck. They may be the result of local dilatation of skin capillaries and abnormal thinness of the skin. They are sometimes called stork bites or telangiectasia. These marks usually fade and disappear altogether. They may be noticeable when the infant blushes, is extremely warm, or becomes excited.
(2) A Hemangioma or strawberry mark is a type of birthmark that is characterized by a dark or bright red raised, rough surface. They do not develop for several days. They may regress spontaneously or may even increase in size. Surgical removal is not recommended. There is a "wait-and-see" attitude advocated before surgical removal.
7-6. CHARACTERISTICS OF THE NEWBORN GASTROINTESTINAL SYSTEM
a. Mouth. The infant's lips should be pink and the tongue smooth and symmetrical. The tongue should not extend or protrude between the lips. The connective tissue attached to the underside of the tongue should not restrict the mobility of the tip of the tongue. The gums may have tooth ridges along them, and rarely a tooth or two may have erupted before birth. The roof of the mouth should be closed, and the uvula should be present. Sometimes there are glistening spots (firm white or grayish-white nodules, usually multiple) on the palate that are referred to as Epstein's pearls. A common site for them is at the junction of the hard and soft palates.
b. Stomach. The capacity of the infant's stomach is about one to two ounces (30 to 60 ml) at birth, but increases rapidly. Milk passes through the infant's stomach almost immediately. The infant is capable of digesting simple carbohydrates and proteins, but has a limited ability to digests fats.
c. Intestines. Irregularity in peristaltic motility slows stomach emptying. Peristaltic increases in the lower ileum, which results in one to six stools a day. The first stools after birth and for three to four days afterwards are called meconium. Meconium is stringy, tenacious, and black and has a tarry texture. With the ingestion of colostrum or formula, a gradual transition occurs. There may be few greenish stools and the stools will gradually become more yellow. Formula stools are lemon yellow and curdy. Breast milk stools are yellow-orange, soft, and more frequent. See figure 7-7.
NOTE: Peristalsis is referred to as progressive wavelike movement that occurs involuntarily in hollow tubes of the body, especially the alimentary canal.

7-7. CHARACTERISTICS OF THE NEWBORN CIRCULATORY SYSTEM
a. Blood Flow. When the umbilical blood stops flowing at birth, sudden pressure differences occur within the circulatory system. These differences cause the blood flowing to the lungs and liver to increase and the blood flowing through the bypass channels to decrease. Peripheral circulation refers to residual cyanosis in hands and feet. This may be apparent for one to two hours after birth and is due to sluggish circulation. Blood is shunted to vital organs immediately after birth.
b. Blood Coagulation. During the first few days of life, the prothrombin level decreases and clotting time in all infants is prolonged. This process is most acute between the second and fifth postnatal days. It can be prevented to a large extent by giving vitamin K to the infant after birth. With the ingestion of food, establishment of digestion, and maturation of the liver, vitamin K is manufactured by the baby and clotting time stabilizes within a week to ten days.
7-8. CHARACTERISTICS OF THE NEWBORN RESPIRATORY SYSTEM
a. Until the infant's first breath of air is taken, the alveoli (air sacs) in the lungs are in an almost complete state of collapsed. The lungs should be in this state because the lung must not fill with amniotic fluid or other liquids. However, the fluid/liquid that flows in the lungs during normal delivery is squeezed or drained from the infant lungs. The major portion of the fluid is absorbed after delivery by the avcolar membranes into the blood capillaries.
b. The most frequent cause of respiratory difficulty in the first few hours of birth has been due to the too liberal use of sedatives, tranquilizers, analgesics, and anesthetics that affect not only the mother, but pass over the placenta to the infant. These drugs make the baby sleepy and disinclined to take the first breath.
7-9. CHARACTERISTICS OF THE NEWBORN ENDOCRINE SYSTEM
The endocrine glands are considered better organized than other systems. Disturbances are most often related to maternally provided hormones (estrogen, luteal, and prolactin) that may cause the following conditions:
a. Vaginal discharge and/or bleeding may occur in female infants. This discharge is white mucoid in color. Bleeding may occur as a result of withdrawal from maternal hormones at the time of birth. There are usually only a few blood spots seen on the diapers. The entire process terminates in one to two days.
b. Enlargement of the mammary glands may occur in both sexes. This is particularly noticeable about the third day of life. Breast secretion may also occur. Swelling usually subsides in two to three weeks. The breast should not be squeezed; it only increases the chances of infection and injuries to the tender tissue.
7-10. CHARACTERISTICS OF THE NEWBORN NEUROMUSCULAR SYSTEM
The newborn infant exhibits remarkable sensory development and an amazing ability for self-organization in social interactions. The infant's muscles are firm and resilient. He has the ability to contract when stimulated, but lacks the ability to control them. He wiggles and stretches, but movements are uncoordinated.
a. Cephalo-Caudal (Head to Toe) in Development. Gross motor development occurs first, followed by finer motor development. Reflex actions present at birth serve the infant until neuromuscular development is improved. Absence of reflex activity often indicates some form of brain damage.
b. Common Infant Reflexes. See figure 7-8.
(1) Rooting. The infant turns his head to the side when the side of his face is touched.
(2) Moro reflex. The infant's total body responds to a startling event. His arms extend out and up, legs flex toward abdomen. This reflex is usually lost by three months of age.
(3) Tonic neck reflex. The infant assumes a fencer's position. His arm and leg on one side is extended, the opposite side is flexed. His head is turned toward extended side. This is not evident after four months of age.

Figure 7-8. Common infant reflexes.
|
|
|
The Brookside Associates Medical Education Division is dedicated to the development and dissemination of medical information that may be useful to medical professionals and those in training to become medical professionals. This website is privately-held and not connected to any governmental agency. The views expressed here are those of the authors, and unless otherwise noted, do not necessarily reflect the views of the Brookside Associates, Ltd., any governmental or private organizations. All writings, discussions, and publications on this website are unclassified.
© 2007 Medical Education Division, Brookside Associates, Ltd. All rights reserved
![]()