|
The ear is the primary organ of hearing. It is divided into three parts: the
external, middle, and inner ear.
External Ear
The external, or outer, ear is composed of two parts, the auricle and the
external auditory canal. The auricle, or pinna, is a cartilaginous structure located on
each side of the head. The auricle collects sound waves from the environment, which are
then conducted by the external auditory canal to the eardrum. The lining of the auditory
canal contains glands that secrete a waxy substance called cerumen. The cerumen aids in
protecting the eardrum against foreign bodies and microorganisms.
The eardrum, or tympanic membrane, is an oval sheet of fibrous epithelial
tissue, 10 mm by 9 mm in size, which stretches across the inner end of the external
auditory canal and separates the outer and middle ear. The sound waves cause the eardrum
to vibrate. This vibration transfers the sounds from the external environment to the
auditory ossicles.
Middle Ear
The middle ear is a cavity in the temporal bone, lined with epithelium. It
contains three auditory ossicles-the malleus (hammer), the incus (anvil), and the stapes
(stirrup)-which transmit vibrations from the tympanic membrane to the fluid in the inner
ear. The malleus is attached to the inner surface of the eardrum and connects with the
incus, which in turn connects with the stapes. The base of the stapes is attached to the
oval window (fenestra ovalis), the membrane-covered opening of the inner ear. These tiny
bones link together to span the middle ear. They are suspended from its bony wall by
ligaments and provide the mechanical means for transmission of sound vibrations to the
inner ear.
The eustachian tube connects the middle ear with the pharynx. It is lined with
a mucous membrane and is about 36 mm long. Its function is to equalize internal and
external air pressure. For example, while riding an elevator in a tall building, you may
experience a feeling of pressure in the ear. This is usually relieved by swallowing, which
opens the eustachian tube and allows the pressurized air to escape and equalize with the
area of lower pressure. Divers who ascend too fast to allow pressure to adjust may
experience rupture of their eardrums. The eustachian tube can also be a pathway for
infection of the middle ear.
Inner Ear
The inner ear is filled with a fluid called endolymph. Sound vibrations that
cause the stapes to move against the oval window create internal ripples that run through
the endolymph. These pressurized ripples move to the cochlea, a small snail-shaped
structure housing the organ of Corti, the hearing organ. The cells protruding from the
organ of Corti are stimulated by the ripples to convert these mechanical vibrations into
nerve impulses, which are relayed through the cochlear (8th cranial) nerve to the auditory
area of the cortex in the temporal lobe of the brain. Here they are interpreted as the
sounds we hear.
Other structures of the inner ear are the three semicircular canals, situated
perpendicular to each other. Movement of the endolymph within the canals, caused by
general body movements, stimulates nerve endings, which report these changes in body
position to the brain, which in turn uses the information to maintain equilibrium.
The round window (fenestra rotunda) is another membranecovered opening of the
inner ear. It contracts the middle ear and flexes to accommodate the inner ear ripples
caused by the stapes.
Examination of the Ear:
Hearing:
- Whisper a word (like baseball) about one foot away from the ear.
- If the patient can’t hear the word, he has at least a 30% hearing loss.
External ear (auricle or pinna)
- Inspect each ear and surrounding tissue for deformity, lumps or skin lesions.
- If ear pain, discharge or inflammation is present, move the auricle up and down and press the
tragus.
- Movement of these structures is painful in acute otitis externa, but not in otitis media.
Ear Canal
- When using the otoscope, grip the auricle firmly while pulling upward, back and slightly out.
- Using the largest speculum that fits, insert it into the ear, holding the otoscope braced against the patient’s head.
- Identify any discharge or foreign bodies, redness or swelling. Cerumen may obscure your view and need removal prior to evaluation of the eardrum.
- In acute otitis externa, the canal is often swollen, narrowed, moist, pale, tender, and filled with debris.
- Inspect the ear drum for color and contour. In acute otitis media, the eardrum is red and bulging. Is the eardrum mobile with valsalva or pneumatic attachment?
Drum (Tympanic Membrane or TM)
- Locate Landmarks: Landmarks are obscured with otitis media and acute perforation.
- Umbo — central bulge where the malleus attaches to the drum.
- Light reflex — a line of light from the umbo pointing forward and down.
- Inspect for perforations; the normal drum is translucent, pearly gray color.
- Handle and short process of the malleus — superior to umbo.
Source:
Operational Medicine 2001, Health
Care in Military Settings, NAVMED P-5139, May 1, 2001, Bureau
of Medicine and Surgery, Department of the Navy, 2300 E Street NW, Washington,
D.C., 20372-5300
|


Tragus Press

Auricle pull
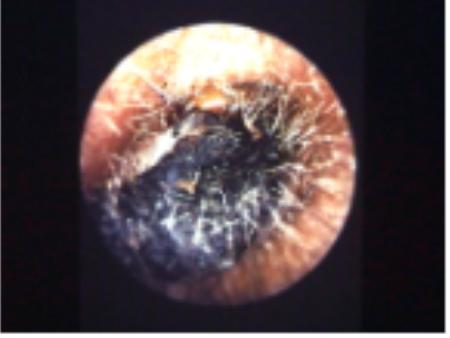
Cerumen Impaction
|