|
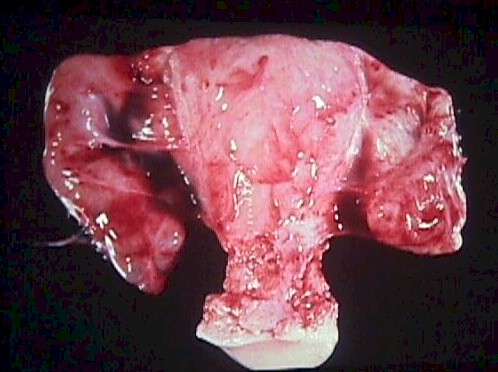
 Pelvic Inflammatory Disease (PID) is a bacterial inflammation of the
fallopian tubes, ovaries, uterus and cervix. Pelvic Inflammatory Disease (PID) is a bacterial inflammation of the
fallopian tubes, ovaries, uterus and cervix.
Initial infections are caused by single-agent STDs, such as gon
orrhea or
chlamydia. Subsequent infections are often caused by multiple non-STD organisms (E. Coli,
Bacteroides, etc.). Responsible organisms include STDs, normal vaginal
inhabitants, and enteric bacteria.
Most cases of PID have no long-term adverse effects, but some have
such serious (or disastrous) consequences as infertility, tubo-ovarian
abscess, and sepsis. Women with a history of PID are at increased risk
for subsequent tubal ectopic pregnancy.
 Symptoms of PID vary from nearly trivial pelvic discomfort and
vaginal discharge to incapacitating abdominal pain with nausea and
vomiting. Leukocytosis, like fever, is variable in cases of PID. The
diagnosis can be based on such imprecise findings as uterine and adnexal
tenderness without other explanation, or such precise findings as
laparoscopic visualization of inflamed tubes with surrounding purulence.
Cervical cultures may or may not be positive. Ultrasound findings may be
normal or may include a generalized haziness due to edema. In more
advanced cases, hydrosalpinx may be seen with ultrasound, CT or MRI. Symptoms of PID vary from nearly trivial pelvic discomfort and
vaginal discharge to incapacitating abdominal pain with nausea and
vomiting. Leukocytosis, like fever, is variable in cases of PID. The
diagnosis can be based on such imprecise findings as uterine and adnexal
tenderness without other explanation, or such precise findings as
laparoscopic visualization of inflamed tubes with surrounding purulence.
Cervical cultures may or may not be positive. Ultrasound findings may be
normal or may include a generalized haziness due to edema. In more
advanced cases, hydrosalpinx may be seen with ultrasound, CT or MRI.
From a clinical management point of view, there are two forms of PID:
-
Mild, and
-
Moderate to Severe
Mild PID
Gradual onset of mild bilateral pelvic pain with purulent vaginal
discharge is the typical complaint. Fever <100.4 and deep dyspareunia are common.
Moderate pain on motion of the cervix and uterus with purulent or
mucopurulent cervical discharge is found on examination. Gram-negative diplococci or
positive chlamydia culture may or may not be present. WBC may be minimally elevated or
normal. These cases are treated aggressively, but usually with oral
medications. Prompt response is expected. Sexual partners should also be
treated.
Moderate to Severe PID
With moderate to severe PID, there is a gradual onset of moderate to
severe bilateral pelvic pain with purulent vaginal discharge, fever >100.4 (38.0),
lassitude, and headache. Symptoms more often occur shortly after the onset or completion
of menses.
Excruciating pain on movement of the cervix and uterus is characteristic
of this condition. Hypoactive bowel sounds, purulent cervical discharge, and abdominal
dissension are often present. Pelvic and abdominal tenderness is always bilateral except
in the presence of an IUD.
Gram-negative diplococci in cervical discharge or positive chlamydia
culture may or may not be present. WBC and ESR are elevated.
These more serious infections require more aggressive management,
often consisting of bedrest, IV fluids, IV antibiotics, and NG suction
if ileus is present. A more gradual recovery is expected and it may be
several weeks before the patient is feeling normal. |

