Uterine Leiomyoma (Fibroid
Tumors of the Uterus)
Uterine leiomyomas are common, benign, smooth muscle tumors of the
uterus. They are found in nearly half of women over age 40 and
infrequently cause problems. Synonyms include Fibroids, Myomas, and
Leiomyomata.
 Fibroids tend to grow under the influence of estrogen,
and regress when the estrogen levels are reduced. Thus, growth
frequently occurs during pregnancy, followed by regression following
delivery. After the onset of menopause, fibroids generally regress. Fibroids tend to grow under the influence of estrogen,
and regress when the estrogen levels are reduced. Thus, growth
frequently occurs during pregnancy, followed by regression following
delivery. After the onset of menopause, fibroids generally regress.
High-dose birth control pills, by virtue of their high estrogen content,
can cause fibroids to grow larger. Low-dose birth control pills, in
contrast, leave circulating estrogen levels the same (or reduced) and do
not stimulate fibroid growth.
 Symptoms Symptoms
Most women with uterine fibroids have no symptoms, but some do. Symptoms
that might be experienced include:
- Heavy menstrual flows: This happens more often with
submucous fibroids (just below the surface of the endometrium) that
expand the cavity size leaving a much larger surface area for
bleeding. Pedunculated fibroids that protrude into the uterine cavity
and also cause menorrhagia by interfering with the normal contractile
mechanisms of the uterus.
- Bleeding between periods: Pedunculated fibroids and
submucosal fibroids can mechanically traumatize the uterine lining,
leading to dysfunctional bleeding.
- Pain: This may take the form of menstrual cramps,
painful intercourse on deep penetration, pain of acute fibroid
degeneration, and chronically inflamed fibroids with a dull, aching or
heaviness that is mostly constant.
- Infertility: Fibroids, depending on their location,
can interfere with fertility.
- Pelvic Pressure: This heaviness in the pelvis is
distracting and annoying
- Stress Urinary Incontinence: The bulk and irregular
proportions of fibroids can distort the pelvic anatomy sufficiently to
interfere with normal urinary retention and release.
- Ureteral Obstruction: If large enough and filling
the pelvis, fibroids can put pressure on and partially obstruct the
ureters, increasing the risk of infection, stones and renal disease.
 Clinical Findings Clinical Findings
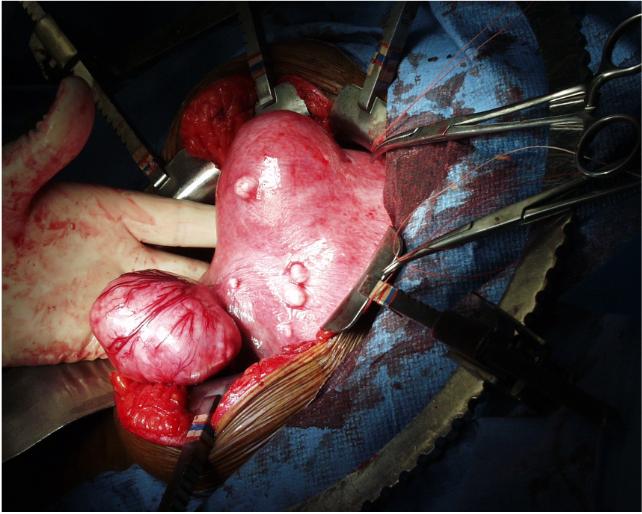
The uterus is irregularly enlarged and usually somewhat asymmetrical. It
may be tender and may assume very large sizes. Unlike the soft uterus
containing a pregnancy or adenomyosis, the fibroid uterus is very firm.
Confirmation of Diagnosis
The diagnosis is usually based on the clinical findings of an enlarged,
irregularly shaped, firm uterus that may or may not be tender.
Sometimes, the diagnosis is unclear and diagnostic tests are used to
delineate the fibroids and rule out other problems. These include:
- Ultrasound: This is a reliable means to show the
fibroids and distinguish between ovarian and uterine growth.
- MRI and CT Scanning: These can be useful, showing,
for example, whether the ureter is obstructed and ruling out bowel
involvement..
- Laparoscopy: Rarely used for diagnostic purposed, it
might occasionally be used for confirming the diagnosis of fibroids
coming from the uterus.
- Histology: As the risk of malignancy in a mass
thought clinically to be a fibroid is <1%, surgical removal solely
to confirm the absence of cancer is only
infrequently undertaken. Factors that could increase your concerns for
this could be rapid growth or other associated symptoms.
 Mangement Options Mangement Options
No single treatment plan is best for all women with fibroids. In
most cases, no treatment at all is necessary. The fibroids are
measured and observed over time, with the expectation that at
menopause, they will regress. However, for those with significant
symptoms, very large fibroids, or rapidly growing fibroids, a number
of treatments can be considered. Important factors in deciding therapy
are the severity of the symptoms, associated symptoms, age, and
preservation of fertility:
-
Hysterectomy: This is the only permanent cure for
fibroids. It provides definitive treatment, but requires major
surgery, abdominal, vaginal or laparoscopic.
- Myomectomy: Removal of just the fibroid, with
conservation of the rest of the uterus. For women who wish to preserve their
childbearing capacity, this option may be the best. Unfortunately, myomectomy is often a more complicated procedure than hysterectomy,
involving longer recovery, greater risk of blood transfusion and
infection.
- Birth Control Pill/Progestins: While these will
not shrink fibroids, they may be effective enough in controlling the
symptoms (particularly bleeding) that the patient can make it
through to menopause.
- GnRH Analogs: Through suppression of the release
of gonadotropins, these effectively reduce estrogen concentration to
menopause or near menopause levels. This has the desired effect of
shrinking the fibroids. Unfortunately, after 6 months, when the GnRH
must be stopped, the fibroids will rapidly re-grow, making this a
temporary treatment. But temporary treatment may be very
satisfactory if the goal is to shrink the fibroids to a more
manageable size prior to surgery. The menopausal symptoms can
usually be controlled with add back estrogen, if desired.
- Embolization: Under interventional radiology
guidance, a catheter is threaded through the uterine arteries and a
bolus of tiny plastic pellets injected. These pellets lodge in the
small arterioles leading to the fibroids, reducing their blood flow
and causing necrosis. Good results have been reported in a limited
number of cases by skilled hands in a few centers. Serious
complications have also been noted, leading to emergency surgery and
life-threatening problems. Whether this approach will prove to be
widely accepted remains to be seen.
Military Settings
Military personnel being generally younger, uterine fibroids are uncommon, and
most are asymptomatic. When they are found, they are clinically identified by
the enlarged, irregularly-shaped uterus, often accompanied by heavy, painful
menstrual flows. While definitive therapy involves surgery, low-dose birth
control pills are usually effective in relieving the symptoms for significant
periods of time. Conventional OCPs can be
very effective, but if symptoms persist, use of continuous OCPs will usually
control the symptoms for months or longer, until definitive therapy can be
safely accomplished. If no medications are available, then bedrest while
bleeding will usually lessen the intensity and duration of the bleeding. |

