
![]()
Multimedia Edition
|
Lesson 4: Vital Signs
|
Two things determine the blood pressure: the rate and force of the heartbeat and the ease with which the blood flows into the small branches of the arteries. When the heart rate or force is increased by exertion or illness, blood pressure increases. If the volume of blood within the circulatory system is reduced (as in hemorrhage), and other factors remain the same, blood pressure decreases.
a. Blood pressure is the pressure exerted by the blood on the walls of the blood vessels within the systemic arterial system. Normal systolic pressure for a young adult is 100 to 120 mmHg (millimeters of mercury); diastolic pressure is about 80. Blood pressure increases gradually with age. Normal systolic pressure for a person 60 years of age is 130 to 140. Hypertension is blood pressure above normal limits (above 140/90); it is a sign of a circulatory problem. Hypotension is blood pressure below normal limits (below 90/60) and may indicate shock. See table 4-3.
|
SYSTOLIC 100 to 140 mmHg DIASTOLIC 60 to 90 mmHG |
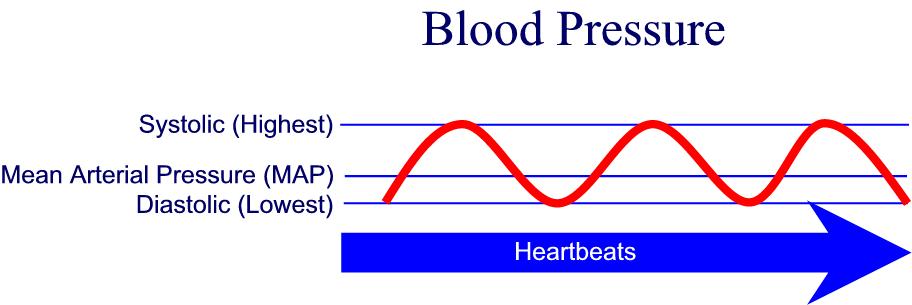
b. Systolic blood pressure is greatest. It is the pressure against the wall of the blood vessels following ventricular contraction. Using the auscultatory (listening) method, the systolic blood pressure is recorded at the highest point at which two consecutive beats are heard (Korotkoff sounds).
c. Diastolic blood pressure is lowest. It is the pressure against the blood vessels when the heart is relaxed before it begins to contract again.
d. The mean arterial pressure (MAP) denotes the average pressure within the arteries. An electronic vital signs monitor can determine and display an accurate average pressure or MAP.
e. Shock or other difficulty is usually indicated by a systolic reading of 80 or less. A diastolic reading over 100 is usually considered dangerously high.
|



4-19. MEASURING BLOOD PRESSURE
Blood pressure is usually measured indirectly using a stethoscope and an instrument called the sphygmomanometer. The most common site is the arm just above the antecubital area, using the brachial artery. Blood pressure may be measured directly by means of a catheter or probe inserted into a blood vessel or the heart.
a. Direct Measurement.
(1) One means of direct blood pressure measurement is to place a special tube in a vein and monitor central venous pressure (CVP). Central venous pressure may be used to determine fluid needs in shock, hemorrhage, or severe burns, to detect pulmonary edema, and to determine the extent of circulatory overload.
(2) Another method of direct blood pressure measurement is internal or invasive monitoring. A large, flexible catheter, such as a Swan-Ganz catheter measures pressures within the heart itself.
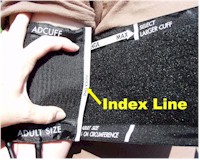
b. Indirect Measurement. The sphygmomanometer (often called a blood pressure apparatus) includes a wide, cloth-covered rubber cuff with two rubber tubes extending from it. One tube is connected to a bulb air pump that has a valve, which can be opened or closed. The other tube is connected to a glass cylinder containing mercury (mercury manometer) or to a dial (aneroid manometer), which attaches to the arm wrap. You obtain the indirect blood pressure reading with the manometer by listening to the heartbeat with a stethoscope.
(1) Cleanse the stethoscope and earpiece with an alcohol wipe before and after the procedure (unless you use your own stethoscope).
(2) Have the patient lie down or rest comfortably in a chair with the arm supported and the palm turned upward to expose the brachial artery on the inside of the elbow.
(3) Let the air out of the cuff. Wrap the cuff firmly around the arm, just far enough above the elbow to leave the space over the brachial artery free, and fasten the clip or Velcro closure.
(4) Find the pulse in the artery and place the stethoscope over the spot where you can feel the strongest pulsations.
(5) Pump the manometer bulb to 20 mm above a possible systolic pressure. Release the valve on the manometer bulb to gradually release air from the cuff.
(6) Note the level on the mercury column or dial at which you first hear a heartbeat. This is the systolic pressure.
(7) Continue gradually releasing air from the cuff. Note the point on the mercury column or dial at which the heartbeat cannot be heard, or at which there is a distinct change in the sound. This is the diastolic pressure.
(8) Release the remaining air from the cuff. Record the blood pressure reading on the patient's chart by writing the systolic pressure above the diastolic pressure. Use only even numbers.
EXAMPLE: BP =
120
80or
120/80
c. Alternate Site for Measurement. If it is impossible to measure the blood pressure in the arm, the leg is used. When blood pressure is taken in the leg, the popliteal space (popliteal artery) is used, and the cuff is applied above the knee. If you measure the blood pressure at any site other than the arm, use the appropriate size cuff and indicate the site on the chart.
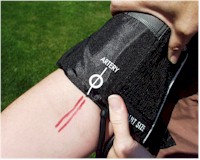
d. Electronic Blood Pressure Apparatus. The cuff of the electronic blood pressure apparatus is applied and manipulated in basically the same manner as with the mercury or aneroid manometer. The cuff is usually inflated and deflated automatically. It is important to place the microphone under the cuff so the arrow that indicates "artery" is in the correct location. Systolic and diastolic pressures will be printed out on the screen within a few seconds.
4-20. FACTORS WHICH INFLUENCE BLOOD PRESSURE VALUES
a. Age. Children normally have lower blood pressure at birth (80/60), which gradually increases until the age of 18 when it becomes equal to the normal adult pressure. Older adults frequently have higher blood pressure due to a decrease in blood vessel elasticity.
b. Sex. Men have higher blood pressure than women of the same age.
c. Body Build. Blood pressure is usually elevated in an obese person.
d. Exercise. Muscular exertion will temporarily elevate the blood pressure. A regular exercise program can eventually decrease the resting blood pressure.
e. Pain. Physical discomfort will usually elevate the blood pressure.
f. Emotional Status. Fear, worry, or excitement can elevate the blood pressure.
g. Disease States and Medication. Some disease conditions and/or the medications influence the blood pressure.
4-21. PRINCIPLES RELATED TO OBTAINING THE BLOOD PRESSURE
a. The patient's arm must be at the level of the heart. If the arm is below the heart, false elevated pressures are obtained. If the arm is above the heart, false lowered blood pressures are obtained.
b. The arm should be supported during the entire procedure to prevent elevation due to muscle contractions used to maintain the position.
c. The cuff and stethoscope should be placed directly on the skin. Light pressure should be applied when placing the stethoscope over the artery.
d. The cuff should be quickly deflated to zero, once the last measurement is heard. Wait a minimum of 30 seconds before measuring the blood pressure again.
|
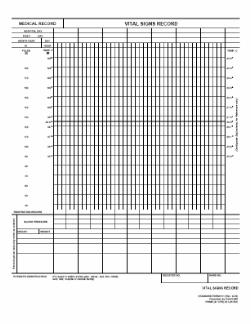
a. A graphic sheet is maintained so that all vital sign readings are easily accessible to members of the health care team. Each reading is recorded as a dot in the proper space, with lines connecting the dots. Readings throughout the patient's illness are indicated across the page in unbroken lines. The form used to graphically record the patient's vital signs in a United States (US) Army hospital is SF 511, Clinical Record--Vital Signs Record.
b. Recording data.
(1) Enter the patient's identification data in the space at the bottom of the form.
(2) Number the "Hospital Day" line of blocks with the day of admission as one, and continue consecutively. Use the "Post-op Day" line as applicable. The day of surgery is the operative day. The day following surgery is noted as the first post-operative day.
(3) Label the day/hour blocks properly.
(4) Represent temperature by dots placed between the columns and rows, and joined by straight lines. If the temperature is other than oral, indicate so by (R) for rectal or (A) for axillary.
(5) Show pulse by use of a circle connected by straight lines.
|
(6) Enter the respiration and blood pressure on the indicated rows below the graphic portion.
(7) Record frequent blood pressure readings on the form's graphic portion by entering an "X" between the columns and rows of dots, at points equivalent to systolic and diastolic levels. Connect the two with a vertical solid line.
(8) Use blank lines at the bottom of the sheet to record special data such as the 24-hour total of the patient's intake and output.
Measuring and recording vital signs is not complicated; however, these are important tasks because these measurements are indicators of functions, which are necessary to sustain life. The patient's current vital signs can be compared with those previously obtained or with normal values and changes in health can be detected and treated quickly.
|
|
|
The Brookside Associates Medical Education Division is dedicated to the development and dissemination of medical information that may be useful to medical professionals and those in training to become medical professionals. This website is privately-held and not connected to any governmental agency. The views expressed here are those of the authors, and unless otherwise noted, do not necessarily reflect the views of the Brookside Associates, Ltd., any governmental or private organizations. All writings, discussions, and publications on this website are unclassified.
© 2007 Medical Education Division, Brookside Associates, Ltd. All rights reserved
![]()