Tinea Capitis
|
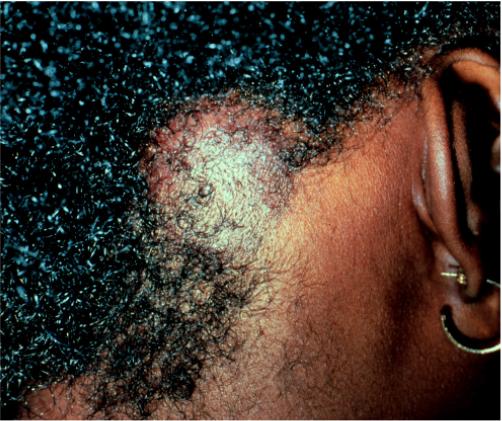
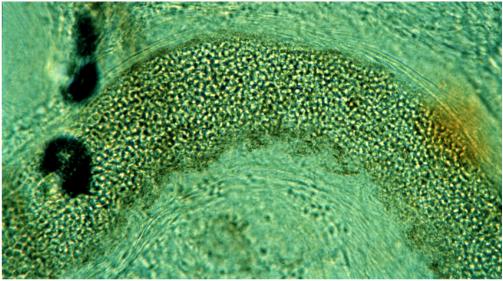
Tinea capitis is classically thought to be a pediatric condition. However, it does occur in the active duty age group, especially black males. The most common cause of tinea capitis in the 1990s is Trichophyton tonsurans. Trichophyton tonsurans infection of the scalp can produce a variable clinical picture. Asymptomatic scaly patches containing tiny black dots with minimal hair loss frequently confused with Alopecia Areata is the most frequent presentation (figure 11) although large, boggy inflamed plaques sometimes occur (figure 12). A Wood's light is of no use to diagnose Trichophyton tonsurans because this organism does not fluoresce. Potassium hydroxide scrapings from the scalp should not be taken from the scale. Instead, they should include the broken fragments of hair or the tiny black dots. Use the tip of an 18-g needle. A curette will function. Be sure to let the preparation digest for several minutes (after gently heating) before viewing. Instead of looking for branching hyphae, look for tiny athrospores (sometimes in chains) within and outside of the hair shaft fragments (figure 13). Therapy of tinea capitis involves systemic antifungals (see below). Topical therapy alone is inadequate, it will not adequately penetrate the hair follicles. The use of an antifungal shampoo such as Selsun, Nizoral, or Head and Shoulders is good adjunctive therapy and will make your patient much less infectious to his/her shipmates. Griseofulvin is still the drug of choice. Oral treatment for at least 10 weeks is necessary. (c) Oral Antifungal
Therapy The use of oral
antifungal therapy is frequently misunderstood by the primary care
provider. For now, griseofulvin is the drug of choice although this
may change in the next year or two. The newer generation of oral
antifungals is quite costly and is frequently unavailable to deployed
units. Griseofulvin Griseofulvin is a
reasonably safe and effective drug in healthy patients if properly
used. Not all griseofulvin preparations are the same. The
bioavailability and doses of micro-size and ultra micro- size forms of
griseofulvin are quite different. Follow the PDR recommendations for
dosing. One exception however, is the need to use the "upper end" of
the dosing scales for tinea capitis. Gastrointestinal side
effects and headache are the most frequent problems with griseofulvin.
These problems can usually be avoided if the drug is given with a
meal, especially with some lipid. A piece of toast with margarine or
oil and vinegar on a salad will provide sufficient fat. Bacon and
eggs are not necessary. Phototoxicity is unusual but reported. Unlike antibacterial
agents, griseofulvin works quite slowly. The deposition of the drug
in newly keratinizing epithelium allows it to work. This takes time
so be patient. Pretreatment liver function tests repeated every month
or two combined with a good follow up monthly will prevent significant
hepatotoxicity. Be aware of the interactions with coumadin and do not
prescribe for patients with porphyria. Ketoconazole This oral form of this
medication is of limited use for treating tinea. This is best
reserved for selected patients with candida or tinea versicolor. Itraconazole (Sporanox) This drug is very
expensive. The use of "pulse" therapy for the treatment of the nails
(tinea unguium) is equally effective as daily therapy in most
patients. Use 200 mg twice a day (with food) for 7 consecutive days
per month repeated for 3 or 4 months. Liver function tests are usually
not needed for healthy patients using this "pulse" regimen. The list
of drug-drug interactions is very long for this medication. Check the
PDR for details. Tebenafine (Lamasil) This medication is also very
expensive. However, it does not have the long list of drug
interactions as itraconazole. The dose is 250 mg daily for 3-4
months. Follow the PDR concerning patient monitoring. |
Written and revised by CAPT Dennis A. Vidmar, MC, USN, Department of Military and Emergency Medicine, and Department of Dermatology, Uniformed Services University of the Health Sciences, Bethesda, MD (1999). Additional images provided by CAPT Vidmar in June, 2000, subsequent to the initial publication of this manual. |


Preface · Administrative Section · Clinical Section
The
General Medical Officer Manual , NAVMEDPUB 5134, January 1, 2000
Bureau
of Medicine and Surgery, Department of the Navy, 2300 E Street NW, Washington, D.C.,
20372-5300
This web version of The General Medical Officer Manual, NAVMEDPUB 5134 is provided by The Brookside Associates Medical Education Division. It contains original contents from the official US Navy version, but has been reformatted for web access and includes advertising and links that were not present in the original version. This web version has not been approved by the Department of the Navy or the Department of Defense. The presence of any advertising on these pages does not constitute an endorsement of that product or service by either the Department of Defense or the Brookside Associates. The Brookside Associates is a private organization, not affiliated with the United States Department of Defense. All material in this version is unclassified. This formatting © 2006 Medical Education Division, Brookside Associates, Ltd. All rights reserved.
Home · Textbooks and Manuals · Videos · Lectures · Distance Learning · Training · Operational Safety · Search
|
|
|
This website is dedicated to the development and dissemination of medical information that may be useful to those who practice Operational Medicine. This website is privately-held and not connected to any governmental agency. The views expressed here are those of the authors, and unless otherwise noted, do not necessarily reflect the views of
the Brookside Associates, Ltd., any governmental or private organizations. All writings, discussions, and publications on this website are unclassified.
© 2006 Medical Education Division, Brookside Associates, Ltd. All rights reserved
Other Brookside Products
![]()