Herpes Simplex (HSV), oral and genital
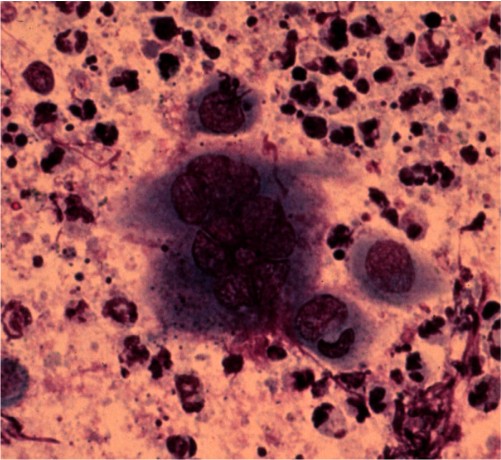
If there is a question of diagnosis, do a Tzanck smear (see technique below). While oral or genital HSV is usually painful, this is not always the case. Be suspicious, especially with penile erosions and ulcers.
Treatment should be individualized.
Topical acyclovir ointment is useless. Tea bag soaks are quite
helpful to dry out the blisters. Have the patient make a cup of tea,
squeeze out the teabag, and then apply the bag to the lesions after it
has cooled. The residual tannic acid in a tea bag is a surprisingly
effective drying agent.
(a) Acyclovir
Oral acyclovir is effective only if
given EARLY in the herpetic episode. In addition, it is not useful
for the patient who gets only the occasional mild episode. Acyclovir
is helpful for patients with an initial outbreak. They are frequently
systemically ill and in pain.
(b) Valacyclovir
This drug is a pro-drug of
acyclovir. Its mechanism of action is identical to acyclovir. The
advantage is that the medication needs to only be used twice a day
instead of five. The dose for recurrent HSV is 500 mg BID for 5
days. The use of 500 mg QD is useful for suppression.
(d)
Other Considerations In
the case of genital HSV, evaluation for concomitant STD should be strongly
considered on an initial visit. STDs are a chummy group and are frequently
transmitted in twos or threes. Look for them!
Although patients are most infectious when they have active lesions, they may
continue to shed virus (albeit at a smaller rate) between outbreaks. As such,
barrier contraception (e.g. condoms) is recommended at all times unless a
couple is trying to conceive.
A couple trying to determine "who gave what to
whom and when" is engaged in a hopeless and psychologically destructive task.
Either partner may have had a dormant infection for weeks, months or even
years. While serologic testing for antibodies to HSV I and II is available, a
positive result is of little clinical utility because over 90 percent of
adults will test positive due to previous exposure to oral or genital HSV. Instructions for performing a Tzank Smear
Written and revised by CAPT Dennis A. Vidmar, MC, USN, Department of Military and Emergency Medicine, and Department of Dermatology, Uniformed Services University of the Health Sciences, Bethesda, MD (1999). Additional images provided by CAPT Vidmar in June, 2000, subsequent to the initial publication of this manual. |



Preface · Administrative Section · Clinical Section
The
General Medical Officer Manual , NAVMEDPUB 5134, January 1, 2000
Bureau
of Medicine and Surgery, Department of the Navy, 2300 E Street NW, Washington, D.C.,
20372-5300
This web version of The General Medical Officer Manual, NAVMEDPUB 5134 is provided by The Brookside Associates Medical Education Division. It contains original contents from the official US Navy version, but has been reformatted for web access and includes advertising and links that were not present in the original version. This web version has not been approved by the Department of the Navy or the Department of Defense. The presence of any advertising on these pages does not constitute an endorsement of that product or service by either the Department of Defense or the Brookside Associates. The Brookside Associates is a private organization, not affiliated with the United States Department of Defense. All material in this version is unclassified. This formatting © 2006 Medical Education Division, Brookside Associates, Ltd. All rights reserved.
Home · Textbooks and Manuals · Videos · Lectures · Distance Learning · Training · Operational Safety · Search
|
|
|
This website is dedicated to the development and dissemination of medical information that may be useful to those who practice Operational Medicine. This website is privately-held and not connected to any governmental agency. The views expressed here are those of the authors, and unless otherwise noted, do not necessarily reflect the views of
the Brookside Associates, Ltd., any governmental or private organizations. All writings, discussions, and publications on this website are unclassified.
© 2006 Medical Education Division, Brookside Associates, Ltd. All rights reserved
Other Brookside Products
![]()