|
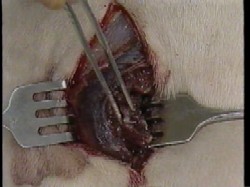
This video was produced by the US
Navy as part of their Operational Medicine CD. The 1-minute clip was
drawn from the longer (31 minute) US Army video, Wound Debridement.
Both show the techniques of
debriding contaminated or infected wounds to speed healing.
The video clip may be freely
downloaded.
|
Following injury from a high velocity
projectile, soft tissue wounds will usually need debridement. This means
removal of dead or dying tissue, foreign bodies (metal or bone fragments),
and other contaminants (pieces of wood, clothing, skin, hair or equipment)
from the wound.
This
debridement is very important:
-
In
addition to the bullet hole itself, high velocity projectiles cause shock
waves that disrupt and destroy tissues as far as several inches from the
missile tract.
-
Incomplete debridement of these damaged tissues increases the risk of
infection and complications including gangrene and death.
-
Incomplete debridement can slow the healing process.
Four
factors are important for a successful debridement:
-
Good Anesthesia
-
An Adequate
Incision
-
Good Assistance
-
Good Lighting
Normally, skin incisions for debridement in the arms and legs are made
longitudinally (parallel to the long bones).
Starting at the wound, use a scalpel to incise the skin , extending it far
enough to obtain good exposure of the injured tissues. Then make another
skin incision, in the opposite direction, again obtaining good exposure. Try
not to incise any deeper than the skin to avoid injuring healthy tissue
underneath the incision. If the wound or your incisions involves a joint, it
is best to obtain consultation (if available) as some incisions over the
joints are better than others.
Don't put your fingers in the wound.
There may be razor sharp metal or glass fragments that can cut you.
After you are through the skin, most surgeons start using curved scissors.
Inserting the closed scissors into the wound tract will help identify the
direction you will need to follow to expose devitalized tissues.
Skin is normally very well vascularized and little, if any
skin will need to be removed. Shreds of skin can be excised, as well as any
crushed, obviously necrotic skin.
Use scissors and tissue forceps (rat-toothed forceps or
pickups with teeth) to undermine and then cut the subcutaneous tissues down
to the peri-muscular fascia. Try to develop each layer, one at a time, as
this will help prevent unnecessary injury and will help you maintain your
orientation, despite the tissue destruction of the wound.
Undermine the fascia with scissors, and then incise it. The
fascia will need to be generously incised in order to expose the underlying
tissue damage. One old expression is: "The Fascia You Should Slash(ia)." If
any fascia is necrotic, excise it and discard it.
As you work your way down through the wound, any loose
foreign bodies should be removed, using forceps to avoid injuring your
fingers. Irrigation fluid (such as normal saline or lactated Ringer's
solution) is very helpful in dislodging clots and other foreign material. It
can be dripped in under pressure from an IV bag, pulsed into the wound using
a syringe, or simply poured in periodically. Gauze sponges help keep the
surgical field clear for you to see.
Once
through the fascia, you will be able to visualize the underlying muscles.
Devitalized muscle is characterized by:
-
Poor color (dark like liver, rather than beefy red)
-
Poor consistency (mushy, like jelly, rather than firm. Normal muscle has
an inherent tone.)
-
Poor contractility (when you pinch it with forceps, nothing happens.
Normal muscle contracts when you pinch it.)
-
Poor circulation (it doesn't bleed when cut)
These are sometimes described as the "Four C's"
-
Color
-
Consistency
-
Contractility
-
Circulation
Devitalized muscle must be removed. Some tissues can get by
for a while with little or no blood supply. Tendons and nerves, if lying
adjacent to other normal tissues, can absorb enough oxygen to survive.
Muscles, however, can't do that. They have a relatively high metabolic rate
and if deprived of oxygen, will die fairly quickly.
Pick up a small piece of devitalized muscle and excise it
with the curved scissors. After it is removed, look at the cut muscle edge.
If it is oozing bright red blood, you have probably excised enough muscle in
that area and you can move to the next area. If the base is not oozing, it
means that you still haven't reached healthy muscle and you you generally
will need to take more out.
The
goal is to remove all dead muscle without taking out very much healthy
muscle.
After completing the superficial soft tissue debridement,
then move to the deeper structures and continue debriding.
You may need to debride through the opposite side of the
wound in order to complete the procedure.
Most oozing will simply stop on its' own or with gentle
direct pressure. Larger bleeders may need to be individually identified,
clamped with a fine hemostat, and ligated. Try to clamp just the bleeding
point, and not the surrounding tissues. Use a fine ligature (thread) to
minimize the amount of foreign material left in the wound.
If you encounter white or yellow fat in the wound, that is a
sign that nerve structures are nearby. Nerves are always well-padded, so
observation of fat should serve as a warning that says, "Watch out. If
you cut here, you may cut a nerve." If the fat is intact, you ordinarily
should leave it alone. Fat doesn't require much oxygen or blood supply and
incising it will only set the patient up for nerve injury.
If at all possible, try not to disrupt nerves or large blood
vessels. The goal is to not just to avoid infection in the traumatized limb,
but to also end up with a functional limb.
After all devitalized tissue is removed, the wound is loosely
packed with gauze, and covered with a loose gauze dressing, The wound is
almost never closed immediately, but left for re-exploration several days
later. Closure may be done then, or even later, via secondary closure,
granulation or skin grafting. A wound that requires debridement is not
likely to be a good candidate for primary closure.
Thus, the basic principles of wound debridement are:
-
Obtain good exposure with good anesthesia, an adequate incision, good
lighting and good assistance.
-
Incise the fascia, exposing the underlying muscle.
-
Excise devitalized muscle until the remaining muscle has good color, tone,
contractility, and circulation.
-
Continue to work downward into the wound, layer by layer, debriding as you
go and trying to avoid the nerves and blood vessels that commonly course
between the muscle layers.
-
Try to preserve as much normal tissue as possible and try not to injure
the nerves.
-
Attempting to close these wounds primarily is usually a very bad idea.
This section was
developed from A1701-89-0142 "JMRTC-Surgical Training. Advanced Trauma Life
Support. Wound Debridement" with LTC Randolf Copeland, MC, USA, Health
Sciences Media Division, US Army Medical Department C&S, Fort Sam Houston,
Texas.
|
