|
This video was produced by the
Brookside Associates in 2008 to assist in orienting medical and nursing students
to this procedure.
The video may be freely
downloaded.
------------------------- Fit the
stethoscope
earpiece to your ears. The tubing should angle slightly upward and toward
the front of your head.
Instruct the patient to take slow, deep breaths
through the mouth while you listen. The breaths should be deep so the air
will completely fill the lungs. They should be slow to prevent
hyperventilation. The mouth should be open to minimize the noisy turbulence
created whenever air moves quickly through the nose.
Listen to each lung in several areas of the back.
Compare the left side to the right side at the same level. Listen to the
apex of each lung over the anterior chest. Avoid trying to listen through
the scapula (shoulder blade) as sound does not conduct well through the
bone. Avoid listening through chest hair or clothing as they introduce
acoustic artifact.
Normal breath sounds are clear.
Crackles (rales) are high-pitched sounds similar to the sound of hairs
being rubbed together. Wheezes have a musical quality to them, reflecting narrowed
air passages vibrating like the reeds on a musical instrument. Pleural
friction rubs are the soft sounds with each breath that resembles two
pieces of leather rubbing against each other. Stridorare the loud, coarse sounds coming from the upper
airway indicating swelling or obstruction. These can be heard without
a stethoscope, some distance from the patient.
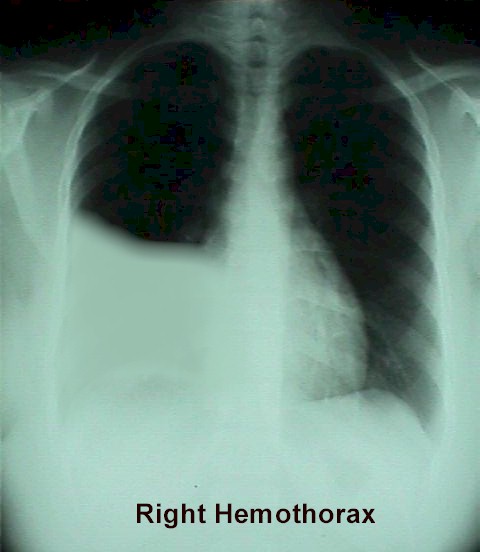
Absent or significantly diminished breath sounds
over part or all of the lung fields may indicate fluid (pleural
effusion, hemothorax) in the chest, or a collapsed lung (air in the
pleural space).
If you are connected to
the Internet, you can hear additional breath sounds at this web site.
From Operational Medicine 2001
|