
Introduction to the Operating Room
LESSON 3: Safety in the Operating Room
3-11
3-11. TRANSPORTING THE PATIENT
a. Discussion. Within any treatment facility, the methods and procedures used for taking a patient into and out of an OR must be implemented in such a way that the patient is not harmed in the process. The methods and procedures in use vary, depending upon the type of medical installation. For example, at an aid station caring for the combat wounded, transporting the patient prepared for surgery may involve little more than lifting the litter onto litter supports and reversing the procedure after surgery.
In a large hospital, a more elaborate procedure is necessary. Regardless of the type of treatment facility, however, the basic purpose of transporting the patient is the same--to move the patient safely in and out of the OR. To this end, the OR specialist transporting patients should observe many precautions.
b. Responsibility of the Operating Room Specialist. In a large hospital, the circulator is often the person who transports the patient to the surgical suite. However, another specialist from the surgical staff may be assigned to transport the patient when the surgery load is heavy, when the distance from nursing unit to OR is long, or when local policy so prescribes. The anesthetist and surgeon always accompany the patient to his post-surgical destination. The specialist is responsible for the patient's safety and well being whenever he is transporting the patient. Therefore, the specialist must know the appropriate procedure for obtaining and transporting the patient. The specialist must know how to recognize and deal with symptoms of distress in the patient and know the location of emergency supplies and equipment along the route. The specialist must never leave the patient unattended on transporting equipment. One person must be with such a patient at all times. In addition, the specialist must account for the patient.
c. Preliminary Preparation.
(1) Preparing the litter.. The specialist's first step in transporting the patient is to "dress" the litter (see figure 3-1). This is to be done in such a way as to ensure the safety and comfort of the patient while in transit. The specialist does this procedure as follows:
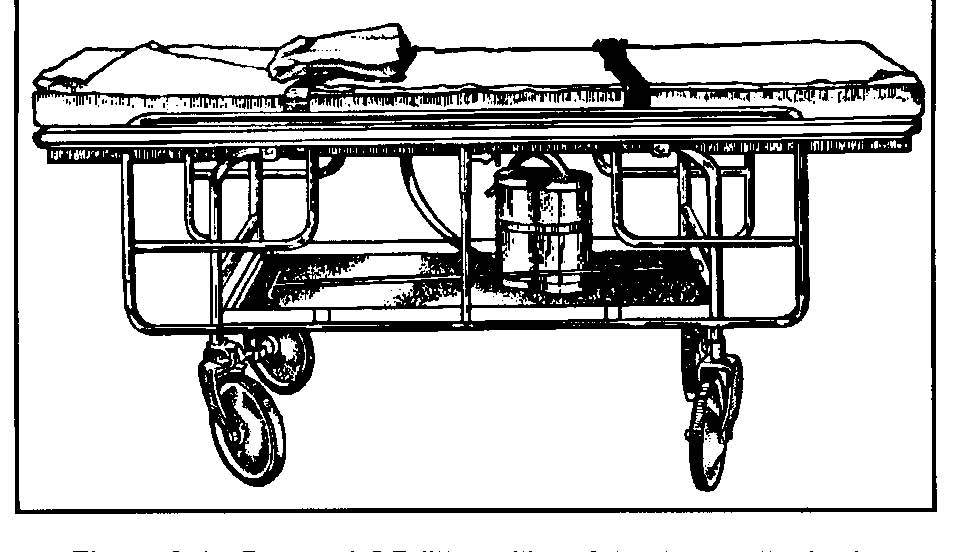
Figure 3-1. Dressed OR litter with safety straps attached.
(a) Place a sheet, folded in half, lengthwise, on the mattress of the litter and tuck it under the mattress all around.
(b) Open fully a second sheet, centered lengthwise, and place it in the litter with one edge at the head of the litter. Now fanfold the sheet from both sides and fold the remaining material at the foot of the mattress.
(c) Place a folded sheet on the litter for use as the cover. If the patient is likely to need additional covering during transport, provide a sufficient number of blankets, made of cotton only. Also place a safety strap, or straps as local policy may require, around the litter (see figure 3-1). Check the OR Schedule and write the patient's name on a piece of paper for reference when on the nursing unit. The OR Supervisor or the OR NCOIC usually directs the specialist to transport the patient.
(2) Accounting for the patient.
(a) Just before leaving the surgical suite, the specialist should draw a circle around the patient's nursing unit number on the OR schedule. This will indicate to other team members that the process for delivering the patient to the OR has been started.
(b) When he brings the patient into the OR, the specialist makes a diagonal mark across the circle.
(c) When the patient is taken from OR, the specialist makes another diagonal mark across the circle so that the final appearance of the nursing unit number is like this--42A. Thus, the patient is accounted for at all times. The particular method may vary, but each OR uses some system to save time and avoid confusion.
d. Identifying the Patient.
(1) Report to the charge nurse. Immediately upon arriving on the nursing unit, the specialist who is to transport the patient reports to the charge nurse, announces the name of the patient, and is told the location of the patient. The Specialist is given the patient's chart, which should contain all laboratory reports, the signed operative permit, and the patient's X-rays. He places these under the foot of the litter mattress.
(2) Specialist's attitude and manner. The specialist must do his best to inspire confidence in the patient. All patients are usually fearful at this time of what may happen to them. Therefore, the specialist must be cordial, considerate, tactful, and accepting of the patient's behavior. A pleasant greeting and explanation of what he is going to do will be appreciated by the patient. Avoid flippancy and apathy.
(3) Confirm identification. Having greeted the patient with a pleasant "good morning" and checked the patient's bed card against the name he has written on the paper, the specialist asks the conscious patient--"What is your name?" (A sedated patient will often agree with any question, which requires only a yes or no answer.) The specialist also checks the hospital identification band (see figure 3-2) worn on the patient's wrist. Local policy may require the charge nurse or someone else on the ward to confirm identity of the patient.
Figure 3-2. Identification band.
(4) Ensure that the patient's preparation is complete. The patient scheduled for surgery is to be attired as prescribed by local policy. The specialist is to put an OR cap on the patient's head in such a way as to cover his hair. Jewelry and prosthetic devices are to be removed by nursing unit personnel and put in a safe place to prevent loss and to protect the patient from possible hazards while he is unconscious. Exceptions may include a patient's wedding ring and religious medal. The ring is to be taped securely to the patient's finger. A religious medal, if the patient desires to wear it, is to be taped directly to the skin. The patient is never to wear such a medal, or any other item around his neck during surgery. An additional exception is a prosthetic device that the surgeon wishes to have left in place. The OR specialist should make a quick but thorough check to see that the patient is in readiness for transportation to the OR.
NOTE: Remember that the patient's wedding ring and/or religious medal may be
taped to his skin ONLY if these objects will NOT interfere with the surgical
area. (See figure 3-3.) If this is the case, local policy will dictate the correct
procedure to follow.
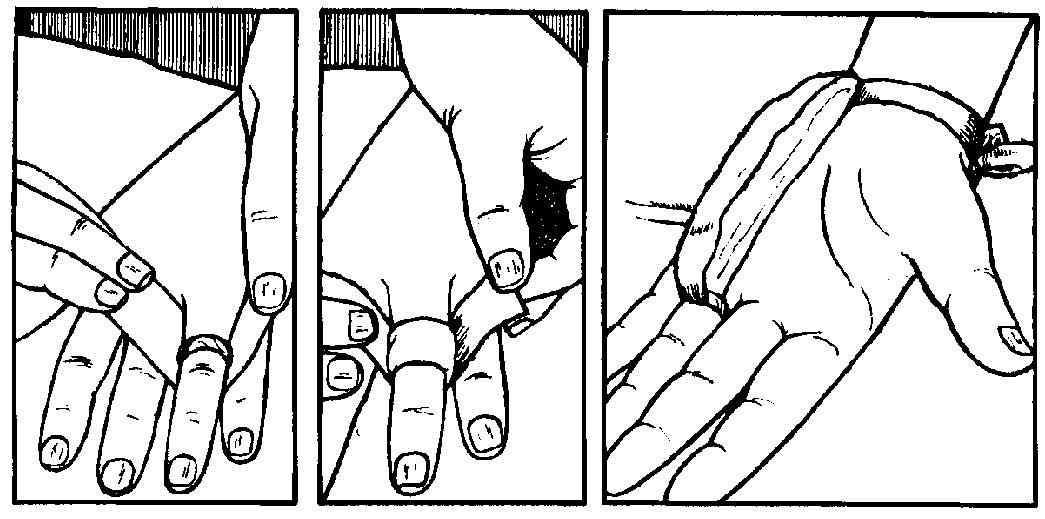
Figure 3-3. Securing wedding ring.
e. Transferring the Patient to the Litter.
(1) If the patient can help himself, the specialist should proceed as follows:
(a) Release the safety straps and cover the patient with the cover sheet from the litter.
(b) Pull the bedclothes to the foot of the bed, leaving the cover sheet over the patient.
(c) Unfold the fan folded litter sheet and move the litter parallel to and against the bed. Check to see that the wheels on the bed are locked.
(d) Stand on the free side of the litter, reach across it and keeping it
steady, place your arms under the patient's shoulders and thighs, and assist him in moving onto the litter. The patient should lie on his back with arms at his side.
(e) The previously fan folded sheet is brought up from the sides and foot to cover the patient completely. Cover the patient additionally if necessary and tuck the covers under the litter mattress. If necessary, use cotton blankets.
(f) Fasten the safety straps snugly over the patient's thighs and the chest, and under and around the litter. Thus, both the patient and the specialist are assured that the patient will not fall off. Do not fasten the straps too tightly, as the patient's circulation may be impaired. The straps should be secured in such a way as to enable the specialist to run his hand, palm down, between the strap and the patient (see figure 3-4).
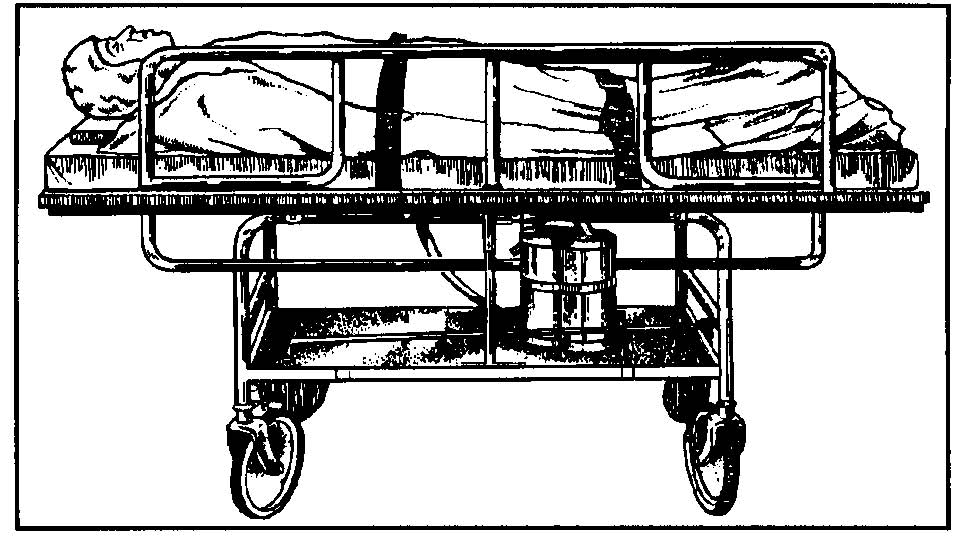
Figure 3-4. Patient ready to be transported.
(Note position of side rail and safety straps.)
(g) Raise and lock litter side rails.
(2) If the patient cannot help himself, he must be lifted onto the litter. A team of at least three people is required to transfer an adult patient from the bed to the litter. They should proceed as follows:
(a) Release the safety straps, cover the patient with the cover sheet, and remove the bed clothing as in (1)(a) and (b) above.
(b) Place the litter at a right angle to the bed, with the head of the litter at the foot of the bed. Unfold the fan folded-litter sheet.
(c) Lock the litter wheels. Make sure that the bed wheels are also locked.
(d) Team member number one. Slide one hand under the patient's head and to his opposite shoulder so that the patient's head rests in the bend of the elbow. Place the other hand under the patient's shoulders and his opposite arms (see figure 3-5A).
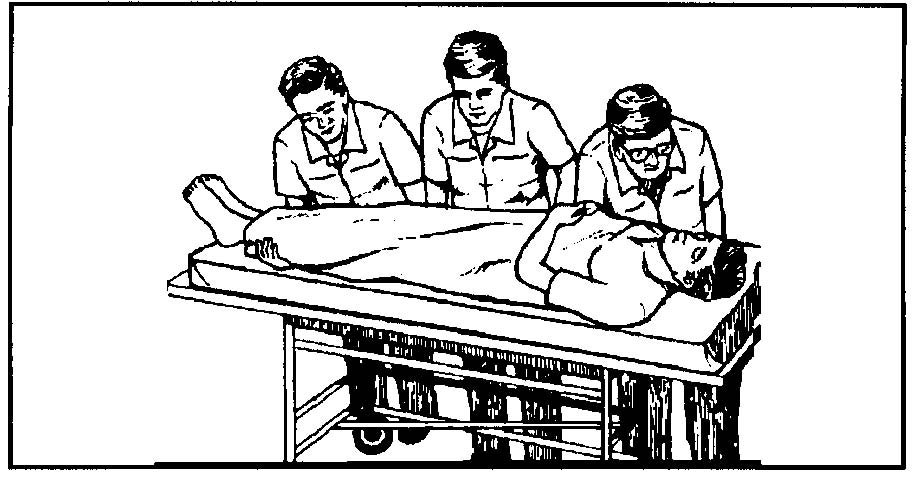
Figure 3-5A. Team member number one positioning patient
for three-man carry, bed to wheeled litter.
(e) Team member No. 2: Place both hands, palm up, under the patient's hips. (See figure 3-5B).
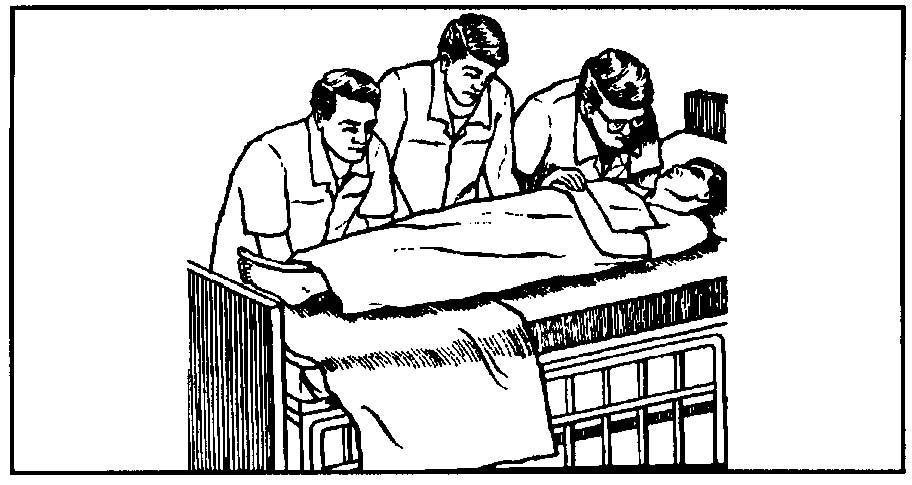
Figure 3-5B. Team member No. 2 positioning patient for three-man carry,
bed to wheeled litter (continued).
(f) Team member No. 3: Place one hand under the patient's thighs and the other under the calves of his legs.
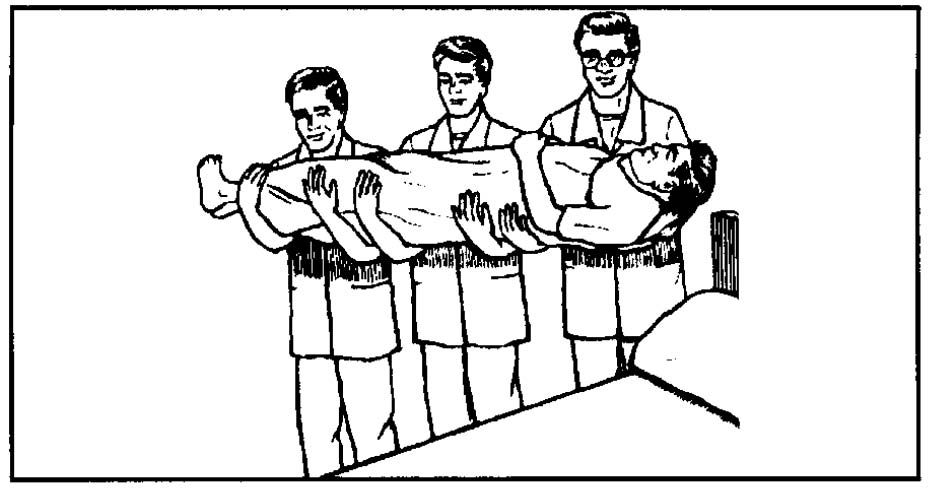
Figure 3-5C. Team members shown doing three-man carry of patient,
bed to wheeled litter (continued).
(NOTE: Cover sheet omitted for visual clarification.)
(g) On signal, draw the patient to the edge of the bed, tilt him slightly toward the team members' chests, and lift him from the bed (see figure 3-5B).
(h) On signal, turn so that the patient's head is toward the head end of the litter, advance to the litter, and carefully place the patient on the litter (see
figure 3-5C).
(i) Cover the patient additionally if necessary and tuck the covers in as described above.
(j) Fasten the safety straps as described in (1)(f) above (see
figure 3-4).
(k) Raise and lock side rails.
(3) Whenever the patient is connected to some kind of apparatus, the specialist should carry out additional safety measures as follows:
(a) If the patient has an IV running, the bottle should be suspended on a litter standard. The litter standard has a plate that, when slipped under the litter mattress will hold the standard upright and support the IV supply bottle. This should be placed near the middle of the litter (never at the head). Thus, if it should fall, it is less likely to injure the patient. The team members lifting a patient with an infusion running should exercise care so as not to disturb the setup. Protection is afforded by splinting the patient's arm. A fourth person may be required to hold the infusion bottle while the patient is being transferred to the litter. If a fourth person is not available, the IV tubing must be clamped off and the bottle hung over the finger or the arm of one of the three people lifting the patient. The bottle is then hung on the standard and the clamp opened. If no litter standard is available, another person must accompany the specialist and the patient to the OR to hold the IV bottle at the same height above the patient as it was in the patient's unit.
(b) The management of drainage equipment will vary with its type and function. If the patient has a urethral catheter connected to a tube leading into a drainage bag, the specialist should clamp the tube. Similar technique is to be used with suction tubing. Drainage will be restarted in the OR if the surgeon desires.
(c) If there is chest drainage, the tubing should be double-clamped on the nursing unit. An assistant should carry the drainage bottles at a level below the height of the patient's chest.
f. Wheeling the Patient. One specialist can safely wheel the patient on a litter if the route to the OR is smooth and does not include steeply inclined ramps and if the patient has no special apparatus attached which requires the attention of an additional person. The specialist is to push the litter ahead of him, guiding it from the
head end. He is to move at a safe pace, being careful not to bump anything or anyone, not to turn corners sharply or otherwise disturb or frighten the patient. When entering the elevator the patient is wheeled in headfirst. The specialist must not smoke while wheeling the patient.
g. Arrival at the Surgical Suite. Upon arrival at the surgical suite, the specialist should report to the anesthesia department and to the OR supervisor or the NCOIC; in addition, as stated above, he should draw a diagonal mark across the patient's nursing unit number on the OR schedule. The specialist remains with the patient (unless he is properly relieved) until the patient is to be transferred onto the operating table. The specialist is then to assist in transferring the patient to the table.
h. Care of the Patient Awaiting Surgery. The patient may be brought to the surgical suite before the scheduled time for his operation, necessitating a wait somewhere outside the OR in which his surgery will be performed. It is important that the patient remains relaxed and comfortable during his wait, since a favorable
environment at this time contributes much to a smoothly conducted, successful operation. Therefore, the OR specialist should place the patient's litter away from glaring overhead lights, into a dimly lit area. The specialist, as well as all of the personnel in the surgical suite, should cooperate in maintaining a quiet atmosphere, because the patient is especially sensitive to noise at this time. Loud talking, laughing, discussion of operative procedures within his hearing, or other inappropriate behavior can frighten the patient and destroy his confidence in the surgical team. In addition to making the patient's environment as calm and serene as possible, the specialist may make the patient more comfortable by placing a pillow under his head and by allowing him to turn on his side; however, first the specialist must ensure that these measures are not contraindicated (made inadvisable).
i. Transferring the Patient to the Operating Table. The patient may be transferred to the table either inside or outside the OR. In either case, the sheet coverings on the patient are loosened while the patient is outside the OR in order to hold to a minimum the fanning of the covers, with their microbial population, in the OR. The patient is transferred with the cover sheet over him.
(1) Outside the operating room. When the patient is transferred outside the OR, the operating table is brought out to the litter. After the patient is transferred, the table is wheeled back into the OR and the wheels of the table are locked.
(2) Inside the operating room. When the patient is placed on the table inside the OR, the litter is wheeled into the OR and placed alongside the table. After the patient is transferred, the litter is wheeled from the room.
j. Procedure During and After Surgery.
(1) Preparation of the litter. As soon as a patient has been transferred from the litter to the operating table and while the patient is still in the OR, the litter is to be stripped, cleaned as necessary, and "dressed" to await further use. These procedures may be carried out by the circulating specialist or by another person assigned by the OR Supervisor or NCOIC. The person who dresses the litter should also see that hand towels and an emesis basin are at hand to accompany the patient to his post-operative destination. Some postoperative patients become nauseated and vomit during transit. The emesis basin and towels are used to keep the patient clean and comfortable.
(2) Delivery of the patient. Upon the completion of surgery, the patient is lifted onto the litter and positioned. The safety straps are fastened, and he is transported to either the recovery room or the nursing unit. Both his position and his destination depend upon the type of anesthetic and the kind of surgery the patient has undergone.
(a) The patient who has been given a general anesthetic should be placed in a lateral recumbent (side-lying) position unless this position is contraindicated by the surgery performed. In which case the patient should be placed either supine (on his back) or prone (on his abdomen), with his head turned to one side. Turning the head to one side facilitates the normal drainage of secretions and helps prevent the aspiration of secretions and vomitus. The endotracheal tube, if one has been inserted, should be left in place and kept free from obstruction until the patient's gag reflex returns. Usually, the anesthesiologist or anesthetist accompanies the patient to the recovery room, and there is assisted by either the circulator or the specialist who assisted with anesthesia during surgery. The patient who has had a spinal anesthetic should be transported to the recovery room in either a dorsal recumbent (supine) position or prone position.
(b) When brought into the recovery room, the patient may be transferred to recovery room equipment or remain on the wheeled litter for care by recovery personnel. (In either case, the specialist should put side rails in place to ensure that the patient will not fall off the bed.) A patient expected to remain in the recovery room for only a short time may afterwards be wheeled to the nursing unit on the same litter on which he was brought to the recovery room. If a lengthy stay in the recovery room is anticipated, the patient is often placed in a recovery room bed immediately after surgery. An arrangement that provides for a minimum number of transfers of the postoperative patient protects the patient who has had spinal or general anesthesia from sudden and dangerous drops in blood pressure.
(c) The trip for the delivery of the patient to the nursing unit may originate in the OR or the recovery room. A patient who has given a local anesthetic or regional block is transported directly from the OR to the nursing unit by an OR specialist. If the distance from the OR to the nursing unit is short, one OR specialist may transport the patient. However, two persons may be assigned when the trip is time-consuming because of either the distance or other factors.
(d) While transporting a patient, the specialist must be continually observant for symptoms of respiratory difficulty, shock, or hemorrhage, and should be ready to employ emergency techniques that are within his capability. He must know the location of emergency equipment such as suction machines and oxygen therapy equipment along the route. He must also be able to summon professional aid and assist with emergency procedures instituted by the MC Officer or the AN Officer who responds to his call for help. Upon arriving on the nursing unit, the specialist is to report to the nursing unit office, return the patient's chart, and request help as needed for transferring the patient onto his bed. The specialist and any designated helpers then wheel the patient to his bed and place him upon it.
k. Other Means of Transporting the Surgical Patient. All pieces of equipment brought from the nursing unit must be damp-dusted with alcohol or as directed before being brought into the OR. This includes the beds, turning frames, and equipment for transporting infants discussed below.
(1) Adjustable (Gatch) bed. The patient may be wheeled to the OR upon his bed. A patient who is seriously ill or one who is to have cardiac or chest surgery is in this way spared the procedure of being transferred to a litter, a procedure that may endanger the life of such a patient. The bed is adjusted to place the patient in the position that is most healthful and comfortable to him. At least two specialists are required to wheel the patient in bed to his destination. The specialists must secure side rails onto the bed and be very careful not to traumatize the patient, either physically or mentally, during transit.
(2) Fracture bed. The surgeon may order that a patient scheduled for orthopedic surgery be transported in his fracture bed. This means of transportation is especially desirable when traction has been applied preoperatively since removing it could put the body out of alignment. At least two specialists are required for transporting a patient in a fracture bed. The specialists must use every precaution during transit to avoid disturbing the traction or otherwise injuring the patient.
(3) Turning frame or reversible bed. Surgeons often order that patients upon Stryker frames or Foster beds be transported on them. The specialist must apply several safety straps before transporting the patient since patients on turning frames are often helpless (because of injuries to the spinal cord or the brain, certain kinds of orthopedic conditions, severe burns, paralysis, or the application of traction). At least two specialists must be available for transporting the patient, and they must take the utmost care to avoid traumatizing the patient.
l. Special Means Used for Infants and Children.
(1) The specialist may be required to wheel a small child or an infant in a pediatric crib or a bassinet. When using either of these methods, two specialists may be required, as cribs and bassinets are quite awkward to handle.
(2) Tiny infants may be brought to the OR in an incubator. An incubator (see figure 3-6) is a small crib unit equipped with an inlet for oxygen, a mechanism for supplying heat, and a temperature-regulating mechanism. The incubator is mounted on a wheeled stand. Oxygen may be supplied by means of either a small cylinder or a large cylinder and is piped into the incubator through a tube. If the oxygen is to be kept running during transport, the specialist must check the liter flow gauge both before and during transit.
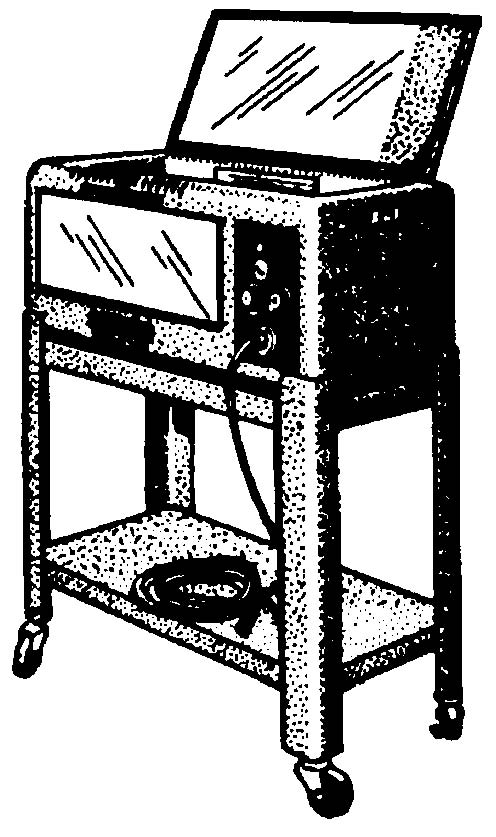
Figure 3-6. Infant incubator.
