
Introduction to the Operating Room
LESSON 1: ORIENTATION
1-21
1-21. ADDITIONAL EQUIPMENT
a. Endoscopy.
(1) General. Endoscopy is a visual examination of the interior of the body cavity, hollow organ, or structure with an endoscope, an instrument designed for direct visual inspection. The endoscope usually is inserted into a natural body orifice, that is, the mouth, anus, or urethra. It may be inserted through a small skin incision and/or trocar puncture, as through the abdominal or vaginal wall. An endoscopic procedure is designated by the anatomic structure to be visualized.
(2) Light source. Illumination within the body cavity is essential for visual acuity. The light source may be through a fiber-optic bundle or from an incandescent light bulb.
(a) Fiber-optic lighting. This is an improved lighting system that illuminates body cavities, including those that cannot be seen with other light sources. Light is conducted through a bundle of thousands of coated glass fibers encased in a plastic sheath. Electric current must be transmitted to the light source connected to the fiber-optic bundle. With fiber-optic lighting, the electric current is entirely external to the patient.
(b) Bulbs screw into the fitting either at the end of a removable light carrier or at the end of the built-in lens system. Electric current is conducted through a single-filament wire to illuminate the tiny incandescent light bulb. A battery box with one or more sets of dry-cell batteries may be used as the power source for light bulbs. Fiber-optic lighting has replaced bulbs in most endoscopes.
(3) Accessories. Accessories such as suction tubes, snares, biopsy forceps, grasping forceps, electrosurgical tips, sponge carriers, and so forth, are used in conjunction with endoscopes. These can be passed through channels in the endoscope to remove fluid or tissue, coagulated bleeding vessels, inject fluid or gas to distend cavities, and so forth. Lensed scopes may be equipped with a still or motion picture camera so organs or lesions can be photographed during the procedure. Some rigid scopes have an obturator, a blunt-tipped rod placed through the lumen of the scope, to permit smooth insertion of the instrument as into the anus. The accessories that will be needed will be determined by the type of endoscope and the purpose of the procedure.
b. Electrosurgical Apparatus. The electrosurgical apparatus (unit) is an electrical machine that has a very high frequency of alternating current. Figure 1-26 shows an electrosurgical apparatus. The surgeon may use the electrosurgical apparatus to do the following procedures: cut body tissue, stop bleeding from small blood vessels (coagulation), destroy abnormal growths such as a wart (fulguration), and sear or dry tissue (desiccation).
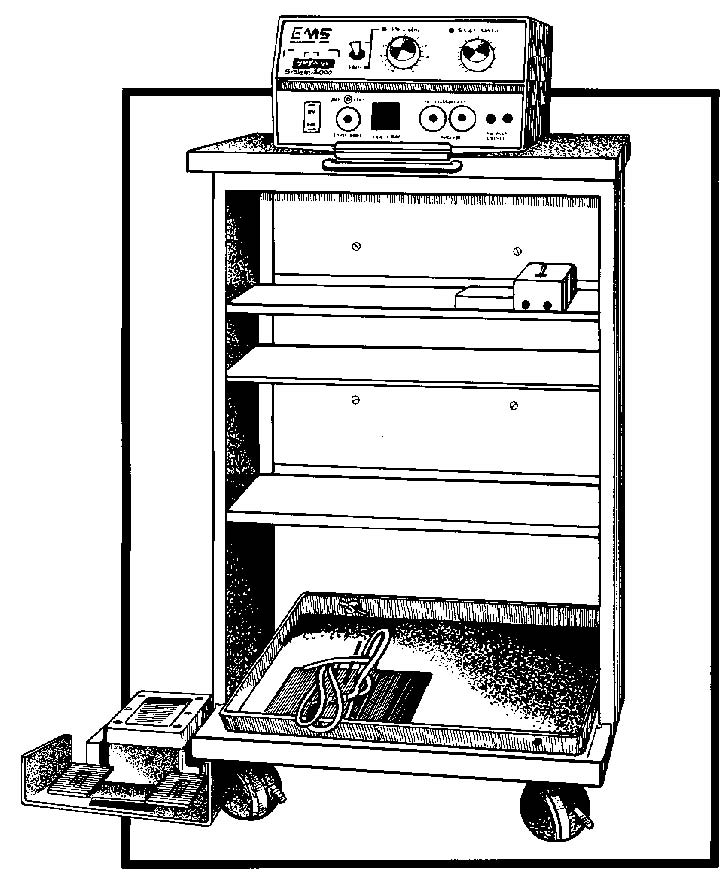
Figure 1-26 Electro surgical apparatus.
(1) Advantages of the use of electro surgery over mechanical (hand) surgery are numerous. A discussion of these follows.
(a) The electrosurgery active electrode (operative tip) can perform two processes simultaneously; it can seal as it cuts. The alternating current makes an incision in an exceedingly fine line. By adjustment of the controls, this unit can also cauterize, or literally cook, the tissue, thus closing (sealing) blood vessels instead of tying each one individually with a suture. These two processes, cutting and sealing, may be done simultaneously or individually. These processes are particularly applicable for use in the presence of cancerous tissue. Removal of malignant growths by mechanical (hand) surgery is dangerous because cells may break off, travel to other parts of the body via the circulatory system, and spread the cancer. However, in electrosurgery, blood vessels are closed as they are cut, preventing the spread of cancer in this way.
(b) Another advantage relates to blood loss. Electrosurgery decreases blood loss. Cauterization is very effective in obtaining hemostasis (arresting the flow of blood). By setting the unit for cauterization, the surgeon need only touch the instrument to the hemostat (clamp which controls bleeding) he has placed on a bleeder and the bleeding is stopped. In mechanical (hand) surgery, each layer of tissue cut requires many hemostats and many ties. Considerable blood is lost while time is taken to tie each bleeder.
(2) The electrosurgerical apparatus has an active electrode and an inactive electrode.
(a) Current passes into the patient's body through an active electrode, the operative tip. A tip is small in area, concentrating the current; hence, it generates considerable heat where the surgeon applies it. The active electrode and its connecting cord are the only parts of the unit sterilized for the operation. This operative tip used by the surgeon is heated only while it is being used; either by a switch on the active electrode handle or by a foot switch, placed near the operating table.
(b) The electrical circuit is completed with the inactive electrode, a large plate made of CRM. This plate is large so that the energy is spread over a large surface area, such as the buttocks, dispersing the current and producing only
negligible heat. The inactive electrode is often placed under the patient's buttocks because of the fleshy, smooth tissue available there which can
provide a good contact. The area used for inactive electrode must be free from scars and excessive hair. Scar tissue is made up of uneven connective tissue, which does not provide good contact. Hair is not conductive and must be removed for a good contact. In addition, bony portions of the body should not be in contact with the inactive electrode because they provide an uneven current distribution, which may lead to burns. Before the inactive electrode is positioned, it should be covered with contact paste (electrocardiograph electrode paste). This paste facilitates passage of electricity. K-Y lubricating jelly should NOT be used because it is nonelectrolytic and will insulate the electrical contact. This will cause current to pass through the thin portions of the K-Y jelly, thus concentrating the current and causing burns to the patient. Disposable plates that conform to the body are also used.
(3) The OR specialist should read the instructions, usually on a plate on the machine or the instruction booklet appropriate to the machine.
(a) The circulator sets up the unsterile parts of the machine since he is the unsterile member of the team. He must set the controls according to the surgeon's orders. The circulator also places the foot pedal conveniently for the surgeon's use.
(b) The scrub sets up the sterile parts and checks the tip to ensure that all parts are present; he inserts the tip into the handle. The scrub hands the end of the cord with the plug to the circulator, who plugs it into the machine.
(c) The unit is tested for proper functioning before the operative procedure begins.
c. Cardiac Arrest Tray.
(1) A sterile cardiac arrest tray is kept in a place easily accessible to the ORs so that it is quickly available should a patient's heart stop beating during the induction of anesthesia or the course of surgery.
(NOTE: The incidence of cardiac arrest is about 1 in 800 general anesthesia.)
The tray contains the instruments necessary for opening the patient's chest and retracting his ribs, thus enabling the surgeon to use his hand to pump the patient's heart. Cardiac arrest is a dire surgical emergency because when the heart stops there is no circulation of blood and therefore no oxygen is available to the tissues. The tissues of the brain are very quickly damaged by anoxia: thus, the time limit for institution of corrective treatment is considered to be from three to five minutes.
(2) In view of the above considerations, Army hospitals require that a preparedness program be in effect. Cardiac arrest trays are therefore located in all areas where anesthesia (either local or general) is administered. All personnel working in such areas must know where the trays are located.
