
Cardiopulmonary Resuscitation
LESSON 3: INITIATE RESCUE BREATHING ON AN ADULT
3-6
3-6. OPEN THE AIRWAY
Once the casualty is in position for rescue breathing, open the casualty's airway using either the head-tilt/chin-lift method or the jaw thrust method. Sometimes an unconscious casualty who is not breathing or breathing in a weak manner will resume normal respiration when his head is positioned correctly and his airway is opened. This is especially true if the casualty's tongue is blocking the airway. The tongue is the most common cause of airway obstruction in unconscious casualties. Repositioning (lifting) the lower jaw forward lifts the tongue away from the back of the throat and unblocks the airway. Establishing an airway should take between 3 and 5 seconds.
NOTE: An unconscious casualty does not "swallow his tongue." The muscles of the tongue simply relax and slide to a lower position which results in the pharynx being blocked.)
a. Head-Tilt/Chin-Lift Method. The head-tilt/chin-lift (figure 3-2) is the preferred method of opening the casualty's airway if a neck fracture is not suspected. In addition, loose dentures can be handled easier using the head-tilt/chin-lift method.
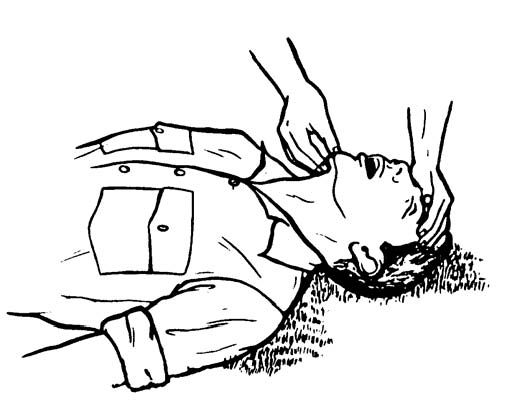
Figure 3-2. Opening the airway: head-tilt/chin-lift method.
(1) Kneel at the side of the casualty's head or shoulders.
(2) Place your hand (the hand closest to the casualty's head) on his forehead.
(3) Apply firm, backward pressure with the palm of your hand. This pressure will cause the casualty's head to tilt back.
(4) Place the fingertips of your other hand under the bony part of his chin, not on the soft flesh under his chin. Pressing on the soft flesh under the chin could result in blocking his airway.
(5) Lift his chin with your fingertips. Continue to lift the lower jaw until his upper and lower teeth are almost brought together. The mouth should not be closed as this could prevent air from entering the casualty's airway.
b. Jaw-thrust Method. The jaw-thrust (figure 3-3) is the preferred method of establishing an airway if you suspect that the casualty has a fractured neck. The jaw-thrust method moves the casualty's tongue forward (away from the airway) without extending his neck.
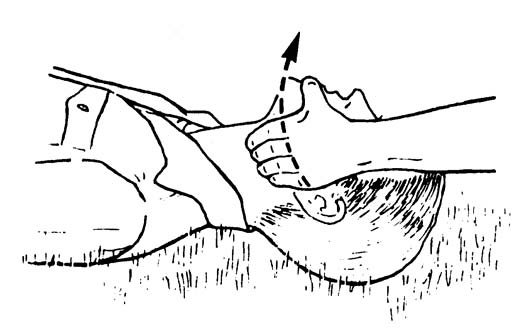
Figure 3-3. Opening the airway: jaw-thrust method.
(1) Kneel behind the casualty's head.
(2) Rest your elbows on the surface on which the casualty is lying.
(3) Place one hand on each side of the casualty's head.
(4) Place the tips of your index and middle fingers under the angles of the casualty's jaw. (This is done on both sides of the casualty's jaw.)
(5) Place your thumbs on the casualty's jaw just below the level of the teeth. The thumbs will keep the casualty's head from turning or tilting during the lift.
(6) Lift the jaw upward with your fingertips. The mouth should not be closed as this could prevent air from entering the casualty's airway. Use your thumb to retract the casualty's lower lip if needed.
(7) If the lift does not open his airway (tongue is still blocking the airway), lift the jaw up a little further. If this is unsuccessful, tilt the casualty's head backward very slightly. In accordance with (IAW) American Heart Association (AHA) guidelines 2005, if you are unable to obtain an airway with the jaw-thrust method, the head-tilt/chin-lift method should be used. The importance of maintaining a patent airway outweighs the risk of spinal damage.
