|
|
Abdominal and Pelvic Pain
When treating a female patient with abdominal pain, I sometimes don't have a clue as to what the problem is. I say this as a board-certified OB-GYN, with more than 20 years in clinical practice, practicing in a 600-bed teaching hospital, with ultrasound, MRI scans, and full lab support. Sometimes all I can say is: "This patient is sick with something."
Sometimes these patients get well before I can figure out the diagnosis. Sometimes these patients get worse and I end up performing surgery and find PID, or endometriosis, or an ovarian cyst or almost any other gynecologic, surgical or medical problem. Sometimes I do laparoscopy and find nothing abnormal, but the pain goes away.
The First Point is: In clinical gynecology, the diagnosis is often unclear. Just because you're unsure of the diagnosis doesn't mean you can't take good care of the patient. Often you must treat the patient before knowing the diagnosis.
The Second Point is: More important than knowing the correct diagnosis is doing the right thing for the patient.
If the patient has pelvic/abdominal pain or tenderness, placing her on bedrest for a few days will usually help and is never the wrong thing to do. For many of your patients, the pain will simply resolve (although you won't know why).
If the patient has a fever (in addition to her pain), I would recommend you give her antibiotics to cover PID. With mild pain and fever, oral antibiotics should work well, so long as they are effective against chlamydia (Doxycycline, tetracycline, erythromycin, Azithromycin , etc.).
If the fever is high or the pain is moderate to severe, I would recommend IV antibiotics (such as clindamycin/gentamicin or cefoxitin or cefotetan or Flagyl/gentamicin) to cover the possibility of pelvic abscess.
If there is no fever, but your patient complains of chronic pelvic pain, a course of oral Doxycycline is wise. Some of these women will be suffering from chlamydia and you may cure them through the use of an antibiotic effective against chlamydia. Others will not improve and will need further evaluation by experienced providers in well-equipped settings.
Any patient complaining of pelvic pain should have a pregnancy test. I am surprised at how often it is positive despite the patient saying "that's impossible."
Most patients complaining of intermittent, chronic pelvic pain will benefit from oral contraceptive pills. BCPs reduce or eliminate most dysmenorrhea and have a favorable influence on other gynecologic problems such as endometriosis, ovarian cysts, and adenomyosis, a benign condition in which the uterine lining grows into the underlying muscle wall, causing pain and heavy periods.
When using BCPs to treat chronic pelvic pain, multiphasic BCPs such as Ortho Novum 7/7/7, Triphasil or Tri-Norinyl have not been as effective as the stronger, monophasic BCPs such as LoOvral, Ortho Novum 1+35 or Demulen 1/35 (in my experience). I believe the reason is that the multiphasic pills, by virtue of their lower dose and changing dosage, do not suppress ovulation as consistently as the higher-dose pills.
If the BCPs do not help or if the patient continues to have pain during her menstrual flow, change the BCP schedule so the patient takes a monophasic (LoOvral, 1+35, etc.) BCP every day. She will:
- not stop at the end of a pack.
- not wait one week before restarting.
- not have a menstrual flow.
If she doesn't have a menstrual flow, she can't get dysmenorrhea. Taken continuously, BCPs are effective and safe. The only important drawback is that she will not have a monthly menstrual flow to reassure her that she is not pregnant.
Because the birth control pills are so very effective in treating dysmenorrhea, the emergence of cyclic pelvic pain while taking BCPs is a worrisome symptom. Endometriosis can cause these symptoms. Happily, birth control pills, particularly if taken continuously, are a very effective treatment for endometriosis. Upon return to a garrison setting, women with pain while taking should be evaluated by an experienced gynecologic clinician.
After a number of months, women on continuous BCPs will usually experience spotting or breakthrough bleeding. It is not dangerous. If this becomes a nuisance, stop the BCPs for one week (she'll have a withdrawal bleed), and then restart the BCPs continuously.
Read more about Birth Control Pills
Any pregnant patient who experiences bleeding should lie still (bedrest) until the bleeding stops for a few days. Then she may be moved to a definitive care setting (hospital). If she is destined to miscarry, having her lie still will not prevent the miscarriage, but it will probably postpone the miscarriage until she can be moved to a safe place where D&C capability is present.
Patients who are less than 20 weeks pregnant and have cramping uterine pain are usually threatening to miscarry. Bedrest is a good idea for all these patients, not because it will prevent the miscarriage, but because it may postpone the miscarriage until the patient is in a location that can deal effectively with any complications. If medical evacuation is not an option, then bedrest will still help the woman tolerate the discomfort of the miscarriage.
Of all women with a threatened abortion, about half will ultimately miscarry and about half will not. In the group who do not miscarry, the remainder of the pregnancy is usually uneventful and the baby will be expected to arrive at full term, alive and without disability.
This is a pregnancy occurring outside the normal location (within the uterus). While these pregnancies will grow briefly, they are not viable and lead to pregnancy loss.
The pregnancy loss can be nearly unnoticed (a "tubal abortion," with the pregnancy expelled out the end of the fallopian tube), but are more often very dramatic, with severe pain and bleeding. If the tube ruptures, extensive and sometimes fatal hemorrhage into the abdominal cavity occurs.
Women with an ectopic pregnancy will almost always have a positive pregnancy test, often have vaginal bleeding, and may or may not have abdominal pain or tenderness. Right shoulder pain is an ominous sign, usually indicating extensive hemorrhage into the abdomen, with irritation of the phrenic nerve which courses along the undersurface of the right hemidiaphragm.
In a hospital setting, a variety of treatments can be considered, including surgery, chemotherapy (methotrexate), and occasionally observation.
In an isolated military setting, bedrest until a prompt medical evacuation to a surgical facility is most appropriate.
Should medical evacuation to a surgical facility not be an available option, treatment is supportive, with IV fluids, bedrest, a MAST suit, and blood transfusions as needed. Most women managed with this supportive treatment will survive treatment, although some will not. Survivors should expect a lengthy, uncomfortable recovery. Oral iron therapy will help restore lost hemoglobin.
Patients who are more than 20 weeks pregnant who have constant pain in the uterus are probably experiencing a placental abruption (premature separation of the placenta), particularly if the uterus is tender. They may or may not have vaginal bleeding.
When hospital care is available, these women are best evaluated by an obstetrician with the technologic resources of electronic fetal monitoring, ultrasound and a sophisticated laboratory testing. In isolated settings, bedrest with the patient lying on her left side and IV hydration are really the only options you have. If the pain improves with bedrest, keep the patient at rest. Consider transport later, after the pain resolves. If the pain shows no evidence of improving with rest, then you will need to transport her sooner since severe placental abruption may be fatal to the patient and/or her baby. Definitive treatment consists of cesarean section and treatment of the coagulopathy (bleeding disorder) that usually accompanies this problem.
If neither definitive therapy (cesarean section) nor medical evacuation are available, the following generalizations can be made:
- With very mild cases, the contractions will usually go away with bedrest and the pregnancy will continue for a while (days to weeks) although early delivery is usually the rule. The ultimate outcome for mother and baby is generally good if the mild abruption is the only significant problem.
- For moderate degrees of placental abruption, the woman usually goes into premature labor and delivers. She generally does well, but the baby may be stillborn or severely incapacitated.
- For severe degrees of placental abruption, if the woman does not deliver very promptly, the abruption will likely prove fatal to her because of the marked coagulopathy that develops. If the baby is not delivered within 10 to 20 or 30 minutes of the severe abruption, it will likely be stillborn.
Under these circumstances, supportive treatment (bedrest, IV fluids, blood transfusions) may be lifesaving.
Any pregnant patient beyond the 20th week of pregnancy who is bleeding should lie still and YOU SHOULD NOT DO A PELVIC EXAMINATION UNLESS INSTRUCTED TO DO SO BY A CONSULTING OBSTETRICIAN. In most cases, the bleeding comes from a small placental abruption and will temporarily resolve with bedrest. Occasionally, the bleeding will be from a "placenta previa," a condition in which the placenta is located immediately behind the cervix. If you perform a pelvic exam on a patient with placenta previa, you may cause massive bleeding which you won't be able to stop without a cesarean section.
Most bleeding in pregnant patients will stop temporarily with bedrest. If a definitive treatment center is close (a brief, smooth ambulance ride), then immediate transport of the patient is best. If a definitive treatment center is distant, it is probably better to stop the bleeding first with bedrest. Move her after a few days when the long and perhaps bumpy transport is less likely to re-start the bleeding. If the bleeding shows no sign of slowing despite bedrest, you may need to begin transport anyway.
Should transport not be an available option:
- Continue the bedrest as long as there is any bleeding. Marginal placenta previas may resolve with time and successful vaginal delivery, while dangerous, can be successful. In this case, pressure from the fetal head on the placenta tends to compress or tamponade the loss of blood from the placenta long enough to achieve a successful delivery.
- In cases of a complete placenta previa, where the placenta totally covers the internal cervical os, maternal death during labor, due to intractable hemorrhage is the rule.
Any woman with an IUD who has any symptoms of pelvic/abdominal pain or abnormal bleeding should first have the IUD removed. Depending on the circumstances, another IUD may be safely inserted at a later time, but the current IUD should be removed. If the pelvic pain is caused by a low-grade infection in the uterus, leaving the IUD in place may lead to a more serious infection and subsequent infertility.
An ovarian cyst is a fluid-filled sac arising from the ovary.
These cysts are common and generally cause no trouble. Each time a woman ovulates, she forms a small ovarian cyst (3.0 cm in diameter or less). Depending on where she is in her menstrual cycle, you may find such a small ovarian follicular cyst. Large cysts (>7.0 cm) are less common and should be followed clinically or with ultrasound.
Occasionally, ovarian cysts may cause a problem by:
- Delaying menstruation
- Rupturing
- Twisting
- Causing pain
95% of ovarian cysts disappear spontaneously, usually after the next menstrual flow. Those that remain and those causing problems are often removed surgically.
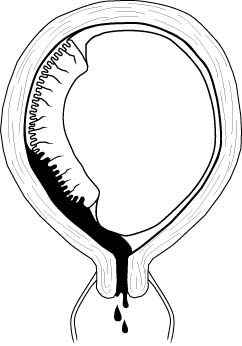
This is an ovarian cyst that has ruptured and spilled its' contents into the abdominal cavity.
If the cyst is small, its' rupture usually occurs unnoticed. If large, or if there is associated bleeding from the torn edges of the cyst, then cyst rupture can be accompanied by pain. The pain is initially one-sided and then spreads to the entire pelvis. If there is a large enough spill of fluid or blood, the patient will complain of right shoulder pain.
Symptoms should resolve with rest alone. Rarely, surgery is necessary to stop continuing bleeding.
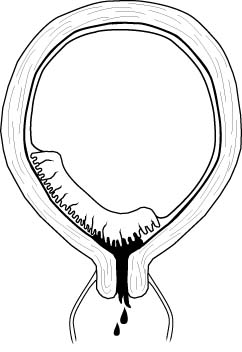
While most of these have no symptoms, they can cause pain, particularly with strenuous exercise or intercourse. Treatment is symptomatic with rest for those with significant pain. The cyst usually ruptures within a month.
Once ruptured, symptoms will gradually subside and no further treatment is necessary. If it doesn't rupture spontaneously, surgery is sometimes performed to remove it. This will relieve the symptoms and prevent torsion.
A torsioned ovarian cyst occurs when the cyst twists on its' vascular stalk, disrupting its' blood supply. The cyst and ovary (and often a portion of the fallopian tube) die and necrose.
Patients with this problem complain of severe unilateral pain with signs of peritonitis (rebound tenderness, rigidity). This problem is often indistinguishable clinically from a pelvic abscess or appendicitis, although an ultrasound scan can be helpful.
Treatment is surgery to remove the necrotic adnexa. If surgery is unavailable, then bedrest, IV fluids and pain medication may result in a satisfactory, though prolonged, recovery. In this suboptimal, non-surgical setting, metabolic acidosis resulting from the tissue necrosis may be the most serious threat. Mortality rates from this condition (without surgery) are in the range of 20%.
Other surgical conditions which may resemble a twisted ovarian cyst (such as appendicitis or ectopic pregnancy) may not have a good outcome if surgery is delayed. For this reason, patients thought to have a torsioned ovarian cyst should be moved to a definitive care setting where surgery is available.
Painful menstrual cramps. These midline, lower abdominal, suprapubic cramps or aches usually begin shortly before the beginning of menses and can persist for a few days into the menstrual flow. Then complete relief occurs and the patient remains pain-free until the next month.
This is not a dangerous condition but can be a powerful nuisance to the patient. The single most effective medication to treat this is oral contraceptive pills (fixed-dose or monophasic BCPs like LoOvral, 1/35s, etc.) Standard doses of non-steroidal anti-inflammatory agents such as naproxen or ibuprofen can be helpful. Exercise, through the release of beta endorphins, is helpful to some.
Patients with endometriosis may also complain of monthly pain. If the symptoms are severe and do not respond to BCPs (cyclic or continuous), or NSAIDs, then endometriosis is usually looked for with diagnostic laparoscopy at an opportune time.
Pain associated with ovulation (from German: "middle pain") which typically occurs at mid-cycle...half way between the menstrual flows.
The pain is either right or left-sided, depending on which ovary released the egg that month. Women do not usually alternate sides, but rather randomly ovulate: sometimes one side, sometimes the other.
The pain, when it occurs, is mild to moderate. There may be some mild peritoneal signs. By the time the patient is examined, the pain is often improving. If the symptoms are severe or last more than a day or two, consider other diagnoses such as ovarian cyst, ectopic pregnancy or endometriosis.
Treatment is supportive. Usually a day or two of rest will see the complete resolution of symptoms. Rarely the symptoms last longer. Any mild analgesic will make them feel better. Birth control pills usually provide complete relief through their inhibition of ovulation.
Intermittent cramping abdominal pain, associated with episodes of constipation or diarrhea, with or without mucous stools.
Patients with this problem give a history of periodically recurring symptoms, often provoked by stress. X-ray evaluation of the abdomen will show no abnormality and all lab studies will be normal. The pain will move from place to place in the abdomen.
Treatment is generally supportive with reduction of stress when that is possible. Avoiding (or treating) constipation or diarrhea is helpful. Non-narcotic analgesics can be given if the pain is quite significant. Antispasmodics are sometimes helpful. Psychoactive drugs are inadvisable unless a specific psychological disorder is present which would be expected to respond to the psychoactive drug.
Acute inflammation of the stomach and intestines, resulting in cramping abdominal pain, distention, nausea, vomiting, diarrhea, fever, and chills. This may be due to bacterial infection, viral infection, or ingestion of a toxic substance (food poisoning).
Patients usually complain of diffuse, cramping abdominal pain with marked GI symptoms. The pain migrates from place to place. Treatment is mostly supportive (rest and observation in mild cases, IV fluids in severe cases) with specific antibiotic therapy when the causative organism is known and sensitive to this approach.
Diverticular disease represents a spectrum of abnormalities ranging from asymptomatic "diverticula" (small outpouchings of the colon) to "diverticulitis" with peritonitis, abscess formation and sometimes perforation of the colon.
Diverticular disease is usually focused in the sigmoid colon in the left lower quadrant, although diverticula can be found in small numbers anywhere along the course of the large and small intestines.
Cramping lower abdominal pain with diarrhea alternating with constipation are symptoms common to those with diverticular disease (and also functional bowel syndrome). If accompanied by fever and elevated white blood count with a mass in the left lower abdomen, "diverticulitis" is likely to be present.
Mild symptoms require only supportive treatment. Diverticulitis often requires IV fluids and antibiotics.
Pelvic Inflammatory Disease (PID) is a bacterial inflammation of the fallopian tubes, ovaries, uterus and cervix.
Initial infections are caused by single-agent STDs, such as gonorrhea or chlamydia. Subsequent infections are often caused by multiple non-STD organisms (E. Coli, Bacteroides, etc.).
From a clinical management point of view, there are two forms of PID:
- Mild, and
- Moderate to Severe
Gradual onset of mild bilateral pelvic pain with purulent vaginal discharge is the typical complaint. Fever <100.4 and deep dyspareunia are common.
Moderate pain on motion of the cervix and uterus with purulent or mucopurulent cervical discharge is found on examination. Gram-negative diplococci or positive chlamydia culture may or may not be present. WBC may be minimally elevated or normal.
Treatment consists of Doxycycline 100 mg PO BID x 10-14 days, plus one of these:
- Cefoxitin 2.0 gm IM with probenecid 1.0 gm PO, OR
- Ceftriaxone 250 mg IM, OR
- Ceftizoxime 1 gm IM, OR
- Cefotaxime 0.5 gm IM
Alternative treatment includes:
- Ofloxacin 400 mg orally twice a day for 14 days, PLUS
- Metronidazole 500 mg orally twice a day for 14 days
For further information, read the CDC Treatment Guidelines for PID
With moderate to severe PID, there is a gradual onset of moderate to severe bilateral pelvic pain with purulent vaginal discharge, fever >100.4 (38.0), lassitude, and headache. Symptoms more often occur shortly after the onset or completion of menses.
Excruciating pain on movement of the cervix and uterus is characteristic of this condition. Hypoactive bowel sounds, purulent cervical discharge, and abdominal dissension are often present. Pelvic and abdominal tenderness is always bilateral except in the presence of an IUD.
Gram-negative diplococci in cervical discharge or positive chlamydia culture may or may not be present. WBC and ESR are elevated.
Treatment consists of bedrest, IV fluids, IV antibiotics, and NG suction if ileus is present. Since surgery may be required, transfer to a definitive surgical facility should be considered.
ANTIBIOTIC REGIMEN: (Center for Disease Control, 1998)
Doxycycline 100 mg PO or IV every 12 hours, PLUS either:
- Cefoxitin, 2.0 gm IV every 6 hours, OR
- Cefotetan, 2.0 gm IV every 12 hours
This is continued for at least 48 hours after clinical improvement. The Doxycycline is continued orally for 10-14 days.
ALTERNATIVE ANTIBIOTIC REGIMEN: (Center for Disease Control, 1998)
- Clindamycin 900 mg IV every 8 hours, PLUS
- Gentamicin, 2.0 mg/kg IV or IM, followed by 1.5 mg/kg IV or IM, every 8 hours
This is continued for at least 48 hours after clinical improvement. After IV therapy is completed, Doxycycline 100 mg PO BID is given orally for 10-14 days.Clindamycin 450 mg PO daily may also be used for this purpose.
ANOTHER ALTERNATIVE ANTIBIOTIC REGIMEN: (Center for Disease Control, 1998)
- Ofloxacin 400 mg IV every 12 hours, PLUS
- Metronidazole 500 mg IV every 8 hours,
ANOTHER ALTERNATIVE ANTIBIOTIC REGIMEN: (Center for Disease Control, 1998)
- Ampicillin/Sulbactam 3 g IV every 6 hours, PLUS
- Doxycycline 100 mg IV or orally every 12 hours.
ANOTHER ALTERNATIVE ANTIBIOTIC REGIMEN: (Center for Disease Control, 1998)
- Ciprofloxacin 200 mg IV every 12 hours, PLUS
- Doxycycline 100 mg IV or orally every 12 hours, PLUS
- Metronidazole 500 mg IV every 8 hours.
For further information, read the CDC Treatment Guidelines for PID
A condition in which fragments of the lining of the uterus are found outside the uterus but within the abdomen. Each month, with menses, these fragments bleed into the abdomen causing pelvic/abdominal pain, scarring, and sometimes infertility.
The classical patient with endometriosis complains of about 6 months of steadily worsening dysmenorrhea, deep dyspareunia, and sometimes painful bowel movements. The physical exam will reveal the adnexal areas and cul-du-sac to be vaguely tender, without masses. When a rectal exam is done and the cervix stretched upward, tender nodules can be felt along the utero-sacral ligaments.
Many medical/surgical treatments are effective. A simple but expedient therapy is taking a low-dose, monophasic BCP each day, without stopping for a menstrual flow. This approach is safe and will postpone menses for months. For cases of mild to moderate endometriosis, this approach is probably as effective as some of the more exotic medications or conservative surgery. In more severe cases, such medications as Lupron or Danazol, with or without surgery, can provide additional relief.
Make sure PID has been ruled out since it can mimic endometriosis.
This condition is characterized by progressive right lower quadrant pain. Nausea and anorexia occur early. Vague pain begins in the periumbilical area and migrates over several hours to McBurney's Point in the right lower quadrant. The patient lies supine with the right hip flexed.
On examination, marked tenderness at McBurney's Point, voluntary guarding, rigidity and rebound tenderness are found. Fever is not common unless appendix is ruptured. Bowel sounds are quiet and no bowel movement will have occurred since the onset of the pain. Motion of the uterus or right adnexa causes marked pain.
X-ray of the abdomen may show an oval, calcified fecalith up to 1-2 cm in diameter in the right lower quadrant of the abdomen. A sentinel loop of gas-filled small bowel next to the appendix may be seen.
The treatment is essentially surgical. Antibiotics may be helpful but are not a substitute for surgery in other than extreme circumstances. If antibiotics alone are used, many patients will live but others will not. Begin treatment with intravenous antibiotics while arranging for transfer to a surgical facility for appendectomy:
- Unasyn 3.0 grams IV every 6 hours PLUS
- Flagyl 500mg IV every 6 hours, OR
- Mefoxin 2 gm IV every 6 hours, PLUS
- Gentamicin 80 mg IV every 8 hours, OR
- Gentamicin 80 mg IV every 8 hours, PLUS
- Flagyl (Metronidazole)
Loading dose: 15 mg /kg infused IV over 1 hour (1 gm or 1,000 mg for a 70 kg adult)
Maintenance dose: 7.5 mg/kg infused IV over 1 hour, every 6 hours (500 mg for a 70 kg adult)
A condition in which a portion of the large or small intestine becomes obstructed.
Patients with bowel obstruction complain of pain, which may be cramping or constant. Abdominal dissension is prominent and patients are constipated. Nausea and vomiting usually accompany this problem. Plain x-rays of the abdomen show a distended, gas-filled loop of intestine proximal to the obstruction. If the problem is not resolved, gangrene and peritonitis develop.
Initial treatment consists of decompression from above with NG suction and support with IV fluids. Partial obstructions are usually relieved with these simple measures. Complete bowel obstruction requires surgery and bowel resection. Without surgery, a complete bowel obstruction would be expected to be fatal. If surgical therapy is unavailable, IV antibiotics should be started while arranging for prompt Medical Evacuation.
When a fibroid tumor of the uterus (leiomyoma) has metabolic needs which exceed its' blood supply, degeneration occurs.
These benign uterine muscle tumors are common (40% of all women by age 40), and generally without symptoms. Occasionally, they cause trouble through excessive bleeding or pain. With degeneration, they become very tender to palpation, but the adnexal structures (tubes and ovaries) are not tender (as they would be with PID).
Treatment is supportive. (bedrest, oral analgesia) Symptoms gradually resolve over 3 weeks. Definitive therapy consists of surgical removal although this is usually unnecessary.
Sooner or later, as many as 5% of all intrauterine devices will become infected. Patients with this problem usually notice mild lower abdominal pain, perhaps a fever and deep dyspareunia. The uterus is tender to touch and one or both adnexa may also be tender.
Treatment consists of removal of the IUD and broad-spectrum antibiotics. If the symptoms are mild and the fever low-grade, oral antibiotics (ampicillin, cephalosporins, tetracycline, etc.) are very suitable. If the patient's fever is high, the symptoms significant or she appears quite ill, IV antibiotics are a better choice (cefoxitin, or metronidazole plus gentamicin, or clindamycin plus gentamicin). If an IUD is present and the patient is complaining of any type of pelvic symptom, it is wisest to remove the IUD, give antibiotics, and then worry about other possible causes for the patient's symptoms.
IUDs can also be rejected without infection. Such patients complain of pelvic pain and possibly bleeding. On pelvic exam, the IUD is seen protruding from the cervix. It should be grasped with an instrument and gently removed. It cannot be saved and should not be pushed back inside.
These bladder infections are quite common. The patient complains of the classical symptoms of urinary frequency, urgency, burning on urination, and pain on completion of urination. Blood, if present, denotes "hemorrhagic cystitis." A tender bladder is virtually diagnostic, although endometriosis can also cause such tenderness.
Treatment consists of:
- Pushing fluids, particularly acid-containing liquids such as cranberry juice or any citric juice (orange, lemon, grapefruit). Acidity inhibits bacterial growth. Vitamin C (Ascorbic acid) can also be used to acidify the urine.
- Any oral broad-spectrum antibiotic, such as:
- Bactrim or Septra
- Cephalosporin
- Amoxicillin
- Tetracycline
- Pyridium for a day will provide immediate relief by anesthetizing the bladder mucosa.
A kidney infection.
These infections are characterized by CVA pain (flank pain) or tenderness, chills, fever, lassitude, and sometimes nausea and vomiting. They may be preceded by cystitis or may come without warning.
Treatment is vigorous antibiotic therapy (frequently IV antibiotics because of the seriousness of the illness) and brisk fluid intake (IV or PO). Severe cases may result in septic shock, DIC and death, even with antibiotic therapy.
Because of the seriousness of this condition, medical evacuation from isolated military settings is usually undertaken. If medical evacuation is not an available option, the prognosis is still reasonably good as the serious complications of pyelonephritis are not common.
Bureau of Medicine and
Surgery |
Operational Obstetrics
& Gynecology - 2nd Edition |
![]()