|
|
|||||||||||||||||||
Red, Watery EyeBackground Red/watery eye means one of the following:
Infection can be either bacterial or viral. Infectious red eye is called “conjunctivitis”. Conjunctivitis is inflammation/redness of the sclera and space under the eyelid. Conjunctiva is resistant to mouth and nose bacteria but is very sensitive to skin sources, especially the genital source. Gonorrhea/Chlamydia causes very serious eye infections. Cold viruses often cause redness too. If both eyes are red consider either viral or allergic etiology. Bacterial infections are usually unilateral then become bilateral in a few days. Infection causes itching, burning, and yellow/greenish discharge or a.m. crusts. Ideal treatment for bacterial conjunctivitis is topical antibiotic ointment that is smeared on the eye and rubbed in every 4 hours. Blurry vision usually resolves in a few minutes. Eye drops are more convenient and should be used every 2 hrs ideally. Total number days of treatment should be about 10 days.
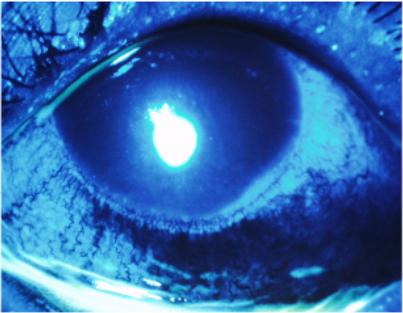
Other things to think about are: acute iritis, narrow angle glaucoma, corneal abrasion, hyphema, and keratitis. These are all painful.
Narrow angle glaucoma Rapid onset, severe pain, decreased vision, halos, fixed mid-dilated pupil; emergency and iv mannitol and acetazolamide, laser treatment. Consult with ophthalmology. Note With common nonvisual painless tearing; consider emotional states, hypersecretion of tears, and blockage of drainage. Tear duct occlusion and pain is due to infection and treat with keflex.
Differential diagnosis:
Discharge present
No discharge, but mild-moderately painful:
No discharge, but moderate to severe pain:
No discharge, and minimal or no pain
This section provided by CAPT Robert B. North, Jr., MC, USN
Home · Military Medicine · Sick Call · Basic Exams · Medical Procedures · Lab and X-ray · The Pharmacy · The Library · Equipment · Patient Transport · Medical Force Protection · Operational Safety · Operational Settings · Special Operations · Humanitarian Missions · Instructions/Orders · Other Agencies · Video Gallery · Forms · Web Links · Acknowledgements · Help · Feedback Approved for public release; Distribution is unlimited.
*This web version is provided by The Brookside Associates, LLC. It contains original contents from the official US Navy NAVMED P-5139, but has been reformatted for web access and includes advertising and links that were not present in the original version. The medical information presented was reviewed and felt to be accurate in 2001. Medical knowledge and practice methods may have changed since that time. Some links may no longer be active. This web version has not been approved by the Department of the Navy or the Department of Defense. The presence of any advertising on these pages does not constitute an endorsement of that product or service by either the US Department of Defense or the Brookside Associates. The Brookside Associates is a private organization, not affiliated with the United States Department of Defense.
© 2015, Brookside Associates, LLC. All rights reserved
|
|
||||||||||||||||||