|
|
Medical Education Division |
Operational Medicine 2001
Technical Manual NEHC-TM6250.98-2 (August 1998)
Home À Military Medicine À Sick Call À Basic Exams À Medical Procedures À Lab and X-ray À The Pharmacy À The Library À Equipment À Patient Transport À Medical Force Protection À Operational Safety À Operational Settings À Special Operations À Humanitarian Missions À Instructions/Orders À Other Agencies À Video Gallery À Phone Consultation À Forms À Web Links À Acknowledgements À Help À Feedback
|
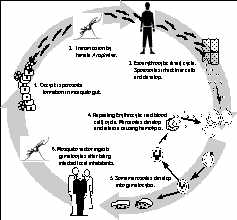
Navy Medical Department Guide to Malaria Prevention and Control Chapter 1: Malaria: Disease, Life Cycle, DistributionDepartment of the Navy Definition Malaria is both an acute and chronic disease caused by protozoa of the genus Plasmodium. Four species cause human malaria: P. falciparum, P. vivax, P. malariae, and P. ovale. The protozoa are transmitted to humans by female mosquitoes of the genus Anopheles. (Transmission can also occur by direct inoculation of infected red blood cells via transfusion, needles, or congenitally). Some signs and symptoms of the illness are high fever, chills, headache, anemia, and splenomegaly. Most serious and fatal complications are caused by P. falciparum. Life Cycle The life cycle of malaria is complex (see Fig. 1-1) with developmental stages and corresponding symptoms differing according to the Plasmodium species involved (see Table 1-1). Sporozoites, the infective stage of plasmodia, are injected from the salivary glands of infected mosquitoes during feeding. Following inoculation, the sporozoites disappear from the blood within 30 minutes. Many are destroyed by white blood cells, but some enter liver cells. Exoerythrocytic Phase. Sporozoites that enter liver cells multiply asexually in a process called exoerythrocytic schizogony. Thousands of uninucleate merozoites form, displacing the nucleus of the liver cell, but causing no inflammatory reaction in the liver. Eventually, invaded liver cells rupture, releasing thousands of merozoites into the bloodstream. This occurs 6 to 16 days after initial infection depending on the infecting Plasmodium species. Dormant or Hypnozoite Phase. All infections due to P. falciparum and P. malariae have a single exoerythrocytic form. All infected liver cells parasitized with P. falciparum and P. malariae rupture and release merozoites at about the same time. In contrast, P. vivax and P. ovale have two exoerythrocytic forms. The primary type develops, causes liver cell rupture, and releases merozoites just as described for P. falciparum and P. malariae. The other form, which develops concurrently, is known as the hypnozoite. Sporozoites that enter liver cells differentiate into hypnozoites that remain dormant for weeks, months, or years. At some future time, the hypnozoites activate and undergo exoerythrocytic schizogony, forming a wave of merozoites that invade the blood and cause a delayed case or a clinical relapse. Erythrocytic Phase. Released merozoites invade red blood cells (erythrocytes), where they develop into trophozoites. After a period of growth, the trophozoites divide and develop, eventually forming 8-24 merozoites in each red blood cell. When this process is complete, the host red blood cells rupture, releasing mature merozoites. The symptoms associated with malaria occur at this point. The merozoites then invade fresh erythrocytes and another generation of parasites develops in the same manner. This process occurs repeatedly during the course of infection and is called eryrthrocytic schizogony. The length of this development cycle differs according to the species of parasite, varying from 48 hours in vivax, ovale, and falciparum malaria, to 72 hours in P. malariae infections. In the early stages of infection there is no characteristic periodicity as groups of parasites develop at different times. The febrile episodes caused are inconsistent. Later, the erythrocytic schizogony development cycle becomes synchronized, and the febrile paroxysms become more consistent. Some merozoites differentiate into sexual forms (female macrogametocytes, male microgametocytes) and develop in invaded red blood cells. Vector Phase. Anopheles mosquitoes feeding on infected hosts ingest sexual forms developing in red blood cells. The female macrogametocytes and male microgametocytes mature in the mosquito's stomach and combine forming a zygote that undergoes mitosis. The products of mitosis are ookinetes, which force themselves between the epithelial cells to the outer surface of the stomach, and form into small spheres called oocysts. The oocysts enlarge as the nucleus divides, eventually rupturing and releasing thousands of motile sporozoites into the body cavity. The sporozoites migrate to the salivary glands, making the female mosquito infective. The vector phase of the life cycle, called sporogony, is complete in 8 to 35 days depending on species and environmental conditions. Environmental Factors. Anopheles mosquitoes are essential for development, multiplication, and spread of plasmodia. Therefore, any area harboring Anopheles mosquitoes may be at risk for malaria transmission. Specific environmental conditions optimal for anopheline mosquito vector and parasite development include temperature between 200 and 300C and a mean relative humidity of 60%. The sporogony phase requires temperatures between 160 and 330C. High relative humidity increases mosquito life-span, thereby increasing the probability of mosquitoes becoming infective. Areas with high rainfall have increased malaria incidence because of an increase in breeding sites. The accompanying high humidity increases survival rates of female anopheline mosquitoes. Elevation, along with cooler temperatures and lower humidity, is also a factor as transmission rarely occurs above 2000-2500 meters. Table 1-1. Selected Characteristics of the Four Species of Human Malaria
Figure 1-1. Malaria Life Cycle
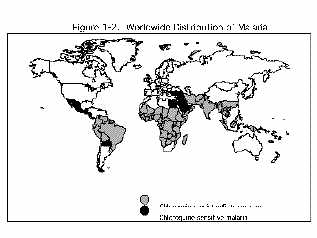
Distribution. The worldwide distribution of malaria is illustrated by the map in Fig 1-2. This is a general representation and not intended for threat assessment or countermeasure planning. Country-specific information can be obtained from the Medical Environmental Disease Intelligence and Countermeasures ("MEDIC") compact disc, and the Navy Environmental and Preventive Medicine Unit responsible for a particular world area. (Further intelligence can be obtained from the agencies listed in Appendix One). Malaria transmission occurs in more than 100 countries. Regions include Africa, Asia, islands of the South, west, and central Pacific Ocean, Latin America, certain Caribbean islands, and Turkey. These areas, all between 450 N and 400 S latitude (see Fig. 1-2), possess tropical or subtropical zones wherein anopheline mosquito habitats exist.
Approved for public release; Distribution is unlimited. The listing of any non-Federal product in this CD is not an endorsement of the product itself, but simply an acknowledgement of the source. Operational Medicine 2001 Health Care in Military Settings
This web version is provided by The Brookside Associates Medical Education Division. It contains original contents from the official US Navy NAVMED P-5139, but has been reformatted for web access and includes advertising and links that were not present in the original version. This web version has not been approved by the Department of the Navy or the Department of Defense. The presence of any advertising on these pages does not constitute an endorsement of that product or service by either the US Department of Defense or the Brookside Associates. The Brookside Associates is a private organization, not affiliated with the United States Department of Defense. |