|
Emergency War Surgery NATO Handbook: Part III: General Considerations of Wound
Management: Chapter XIX: Wounds and Injuries of Bones and Joints
Fractures
United States Department of Defense
In the early stages of treatment, certain principles of war wound management should be
adhered to:
-
The neurovascular status of all injured extremities must be accurately established and
recorded.
-
All open fractures require open debridement and irrigation.
-
The fractures should be reduced and aligned as accurately as possible and initially
splinted in some fashion. As previously stated, the neurovascular status of the extremity
must be established and care must be taken not to compromise the vascular status of the
extremity. If fracture reduction results in circulatory insufficiency, the fracture must
be repositioned and/or the cause of circulatory insufficiency delineated. Biplanar
radiographs are desirable to optimally treat any fracture. It should be kept in mind that
the primary objective in management of extremity wounds is to optimize the situation such
that early wound healing can be obtained, infection prevented, and function restored.
-
Internal fixation of fractures resulting from war wounds is generally contraindicated in
the initial stage of wound management. While there are some exceptions, this should be
considered a generally universal principle. Fractures in extremities where vascular
repairs have been performed are no exception; past combat experience has demonstrated that
traction or other forms of external immobilization can be utilized with vascular repairs.
The addition of internal fixation material to a wound containing a vascular repair results
in an unacceptably high risk of infection and breakdown of the vascular repair.
-
Fractures can be stabilized by the use of splints, circular dressings, pins incorporated
in plaster casts (Figure 25A), or external fixators (Figure 25B). An external fixator should only be applied
only by a surgeon familiar with its indications, application, and potential complications.
The fixator can be extremely useful in the management of large open wounds in which there
has been considerable bone or soft tissue loss or where vascular repair is to be
performed. The advantages in these types of situations are rapid application, ability to
maintain length and position, the ease of access to the wound for dressing changes and
repeat wound debridement, and control of pain because of the stability provided. The rigid
fixation attained frees adjacent joints that would be immobilized in plaster casts and
eliminates the additional weight of the cast, allowing crutch ambulation or transportation
in a sitting position in many patients who would otherwise be litterbound. Additional uses
are the control of hemorrhage in displaced pelvic fractures, and the care and mobilization
of patients with humeral, pelvic or femoral fractures with associated chest or abdominal
wounds. Sufficient rigidity can be obtained in most longbone fractures with the use of a
single frame configuration, consisting of one longitudinal bar attached by two or three
pins distal and proximal to the fracture, to, allow early care and transportation. The use
of half-pins, which pass through the soft tissues on one side to engage the bone but do
not penetrate the soft tissues on the opposite side, minimize the risk to adjacent nerves,
vessels, and muscles. Predrilling the bone with a drill bit and daily local pin care
minimize the complications of pin loosening and pin tract infection.
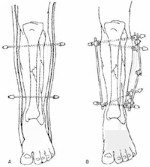
Figure 25.
-
A circular plaster dressing (cast) is applied for immobilization of the joints above and
below a fracture Once applied it must be immediately bivalved to, the skin. A monovalved
cast has no place in the early treatment of a combat casualty. Bivalving the cast for
transportation and evacuation is mandatory. Plaster casts should be marked with
identifying information pertinent to the underlying injury and the date of cast
application for use during transit and by receiving personnel. In general, plaster
splinting is inadequate for anything other than temporary field immobilization. If a spica
cast is constructed, one should avoid making the cast much wider than a standard litter;
this will facilitate movement during medical evacuation.
-
When skeletal traction is employed, Steinmann pins are preferable to Kirschner wires.
They can be easily incorporated into the plaster cast for evacuation and are less likely
to bend. In general, the larger diameter pins should be utilized to prevent loosening and
pin traction infection. Incorporation of traction bows into the cast is unnecessary.
-
Fractures of the humerus or injuries to the shoulder girdle, with or without brachial
artery repairs, are best transported in a Velpeau dressing with the extremity strapped
across the chest; a "sling and swath" can be substituted if necessary (Figure 26).

Figure 26.
-
Elevation of an injured extremity facilitates venous return and minimizes swelling. Ice,
when available, can also be applied in the early injury phase to help control swelling and
make the patient more comfortable. The neurovascular status of the extremity should be
carefully monitored after treatment, and in injuries of both the forearm and the leg the
surgeon must be constantly alert to insure early recognition of compartment syndrome
-
When plaster casts or splints are utilized, particularly in the patient with impaired
sensation, vigilance must be maintained to prevent skin breakdown from excessive cast
pressure Complaints of pain under the cast must not and cannot be ignored. Patients in
spica casts should be turned at intervals to prevent pressure sores over the sacrum and
other bony prominences. Cast pressure I can be minimized by the use of properly padded and
applied plaster.
-
The possibility of fat embolization should be considered in all patients with long-bone
fractures. This is particularly true in patients developing signs of cerebral or pulmonary
dysfunction. Adequate oxygenation is fundamental in the treatment of fat embolism syndrome
and frequently requires the use of mechanical ventilation and positive-end-expiratory
pressures. At the present time there is no hard evidence that validates the efficacy of
intravenous alcohol, heparin, or steroids in the treatment of this primarily respiratory
syndrome Treatment consists of supporting the patient's respiratory function.
-
Preferred regional splinting is as follows:
-
The shoulder joint and humerus, depending on the injury, can be splinted or
immobilized in several manners. As previously noted, a sling and swath or Velpeau-type of
dressing is satisfactory for many injuries, A well-padded, plaster. shoulder spica for
more significant injuries provides better support during transportation. The shoulder
spica cast is extended to include the forearm but not the wrist. An external fixator
applied on the lateral aspect of the humerus with half-pins is a useful alternative to the
shoulder spica or in those with associated chest wounds.
-
The elbow joint and forearm is normally immobilized with a plaster cast, with the elbow
at approximately 90░ of flexion and the wrist and forearm in a neutral position. The
plaster extends from the proximal palmar crease to the axilla. A sling or a collar and
cuff should be used to support the cast and will increase patient's mobility and comfort.
-
If the injury is limited to the wrist itself, the plaster extends from just below the
elbow to the proximal palmar crease (short arm, cast). The wrist should be hold in a
position of approximately 30░ of dorsiflexion. If the thumb is incorporated, it should be
positioned such that the digits can oppose the distal thumb. The hand should be
immobilized with the metacarpal-phalangeal joints flexed and the interphalangeal joints
extended when possible An unaffected digit should not be incorporated into the splint or
dressing. An external fixator or pins incorporated in a short arm plaster cast are
especially useful to prevent shortening in severely comminuted fractures and those with
bone loss.
-
To immobilize the hip joint or a femoral fracture, a bilateral plaster spica extending
from the axilla to the toes on the affected side can be used. The knee should not be
immobilized in hyperextension nor should it be immobilized beyond 10-15░ of flexion. The
spica extends to just proximal of the knee on the unaffected side. When the spica includes
the foot, care must be taken that the normal arch of the foot is maintained and that the
foot is not held either in inversion or eversion. When a cast includes the toes, plaster
must be trimmed away on the dorsum of the foot to a point just proximal to the base of the
toes, thereby permitting the toes to move freely and protecting them from further injury.
This precaution permits periodic evaluation of the distal neurovascular status. An
external fixator applied on the lateral aspect of the femur with half-pins is especially
useful in open femoral fractures. In fractures of the pelvis or hip associated with
abdominal or perineal injuries, a pelvic frame alone, or one attached to a femoral frame,
greatly aids nursing and wound care
-
To immobilize the lower leg and ankle extend the cast from the groin to the toes. The
knee is immobilized with slight flexion avoiding hyperextension or full extension. The
foot is placed in neutral dorsiflexion (at a right angle to the leg). The same care is
taken with respect to the foot as was described in the paragraph above. A single frame
applied to the anterior tibia with half-pins allows mobilization of the ankle and knee
with crutch ambulation, while maintaining length and easy wound access.
-
A plaster cast for the foot and ankle is applied from just below the knee to include the
toes as previously described (with the foot in neutral). Care must be taken that excessive
pressure is not placed on the peroneal nerve which courses just below the lateral aspect
of the fibular head.
-
joints not immobilized should be actively exercised on a frequent basis.
Approved for public release; Distribution is unlimited.
The listing of any non-Federal product in this CD is not an
endorsement of the product itself, but simply an acknowledgement of the source.
Operational Medicine 2001
Health Care in Military Settings
Bureau of Medicine and Surgery
Department of the Navy
2300 E Street NW
Washington, D.C
20372-5300 |
Operational Medicine
Health Care in Military Settings
CAPT Michael John Hughey, MC, USNR
NAVMED P-5139
January 1, 2001 |
United States Special Operations Command
7701 Tampa Point Blvd.
MacDill AFB, Florida
33621-5323 |
This web version is provided by
The Brookside Associates Medical Education Division.
It contains original contents from the official US Navy NAVMED P-5139, but has
been reformatted for web access and includes advertising and links that were not
present in the original version. This web version has not been approved by the
Department of the Navy or the Department of Defense. The presence of any
advertising on these pages does not constitute an endorsement of that product or
service by either the US Department of Defense or the Brookside Associates. The
Brookside Associates is a private organization, not affiliated with the United
States Department of Defense.
Contact Us À À
Other Brookside
Products
|