|
|
Medical Education Division |
Operational Medicine 2001
Second United States Revision of The Emergency War Surgery NATO
Handbook
United States Department of Defense
Home À Military Medicine À Sick Call À Basic Exams À Medical Procedures À Lab and X-ray À The Pharmacy À The Library À Equipment À Patient Transport À Medical Force Protection À Operational Safety À Operational Settings À Special Operations À Humanitarian Missions À Instructions/Orders À Other Agencies À Video Gallery À Phone Consultation À Forms À Web Links À Acknowledgements À Help À Feedback
|
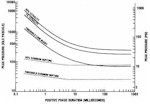
Emergency War Surgery NATO Handbook: Part I: Types of Wounds and Injuries: Chapter V: Blast Injuries Pathology of Primary Blast InjuryUnited States Department of Defense Primary blast injury is seen almost exclusively in gas containing organs: the ear and the respiratory and gastrointestinal tracts. Of the three organ systems, the ear is the most sensitive. The pinna and the external canal collect and in some cases, amplify pressure signals so that the tympanic membrane, converting acoustic energy to mechanical displacement, is displaced into the middle ear. At pressures of approximately 35 kiloPascals (kPa, with 7 kPa equalling 1 pound per square inch), the human eardrum may rupture (Figure 18). Above 100 kPa, almost all eardrums will be ruptured. The eardrum generally perforates inferiorly in the pars tensa but there may be hemorrhage into the membrane without rupture. At higher pressures, the drum may be almost obliterated and the ossicles can be dislocated or fractured. Vestibular function is usually not affected. Injury to the lung is the cause of the greatest morbidity and mortality. Grossly, one sees diffuse, pleurally-based pulmonary contusions with a stiffened, heavy lung. The costal surface may show transverse stripes called "rib markings" which, in fact, are more closely associated with intercostal spaces. Lung weights may be two or three times normal. Pleural rents or blebs may result in pneumothorax, hemothorax, or mediastinal extravasation of air. Rib fractures or evidence of significant chest wall damage are not seen in the absence of other mechanisms of trauma. Microscopically, the hemorrhage is mainly intra-alveolar with some perivascular or peribronchial disruption and bleeding. Alveolar walls are torn, sometimes producing giant blood-filled alveolar spaces. Alveolar-pulmonary venous communications, the source of air emboli within the arterial circulation, are created. These fistulae are responsible for most of the early mortality resulting from primary blast injury. Critical vascular beds in the central nervous or coronary arterial circulations can be occluded by entrained air emboli with subsequent disastrous results. The gastrointestinal tract may be damaged wherever there are collections of gas. Injury to the gut is particularly severe in underwater blasts. While hollow visceral injury is also present in airblast, it is generally overshadowed by the more dramatic presentation of air emboli or acute respiratory insufficiency. The colon is the hollow viscus most commonly disrupted. Gastric injuries are usually less common and less severe. Rarely, one encounters rupture of the spleen or liver in the absence of superimposed blunt abdominal trauma. Pathologically, injuries to the bowel range from subserosal or intramural hemorrhage to frank rupture. The natural history of such bowel wall hemotomas is not known, but it is clear that some can progress to perforation during the post-injury course.
Approved for public release; Distribution is unlimited. The listing of any non-Federal product in this CD is not an endorsement of the product itself, but simply an acknowledgement of the source. Operational Medicine 2001 Health Care in Military Settings
This web version is provided by The Brookside Associates Medical Education Division. It contains original contents from the official US Navy NAVMED P-5139, but has been reformatted for web access and includes advertising and links that were not present in the original version. This web version has not been approved by the Department of the Navy or the Department of Defense. The presence of any advertising on these pages does not constitute an endorsement of that product or service by either the US Department of Defense or the Brookside Associates. The Brookside Associates is a private organization, not affiliated with the United States Department of Defense. |