|
|
Medical Education Division |
Operational Medicine 2001
Second United States Revision of The Emergency War Surgery NATO
Handbook
United States Department of Defense
Home À Military Medicine À Sick Call À Basic Exams À Medical Procedures À Lab and X-ray À The Pharmacy À The Library À Equipment À Patient Transport À Medical Force Protection À Operational Safety À Operational Settings À Special Operations À Humanitarian Missions À Instructions/Orders À Other Agencies À Video Gallery À Phone Consultation À Forms À Web Links À Acknowledgements À Help À Feedback
|
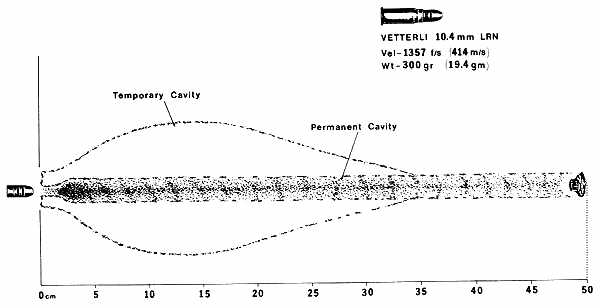
Emergency War Surgery NATO Handbook: Part I: Types of Wounds and Injuries: Chapter II: Missile-Caused Wounds IntroductionUnited States Department of Defense Previous contributions to earlier editions of this handbook devoted considerable effort to differentiating between the magnitude of injury caused by "ordinary" versus "high" velocity missile wounds. To a certain extent, as a result of experience gained in recent conflicts and to a greater extent based on wound ballistic research performed over the past decade, new and somewhat different concepts are evolving. One very fundamental concept is that the high-velocity wound is not necessarily a totally different entity, as had been previously thought. Certain misconceptions continue to be associated with the high-velocity projectile. One misconception concerns the very development of high-velocity weapons. The explanation usually encountered is that these weapons were developed to deliver greater wounding power and higher lethality. Proponents offer the kinetic energy formula in support of their position. Weapons developers state that the real reason that certain countries shifted to low weight, high-velocity projectiles was that their soldiers (who were not the best marksmen) tended to conserve their ammunition and were not discharging their weapons until the enemy was close at hand. It was reasoned that an automatic weapon would obviate some of these shortcomings. From a practical standpoint, the automatic weapon, with its increased requirement for ammunition, necessitated lighter weight ammunition. To compensate for the loss in missile mass, if wounding power was to be maintained, it was necessary to increase missile velocity. These tradeoffs resulted in considerably less recoil, making it easier to maintain the sight picture on repetitive shots, resulting in increased accuracy. The lighter cartridge allowed the individual infantryman to carry the increase in basic load of ammunition (more rounds, same weight) and allowed the maneuver element to present the enemy with greater and more sustained firepower. These are important considerations as the spectrum of warfare shifts more to the left, such as with guerilla-type warfare in which small units engage one another at isolated points, usually at considerable distances from strong points that offer safe haven and resupply. In circumstances such as these, the ability to carry double or triple the basic ammunition load allows small units to take advantage of the increased and sustained firepower that lighter, higher velocity missiles offer. It was for this reason that the current generation of high-velocity weapons was designed, rather than to develop a weapon that inflicts a more severe wound. It is vigorously affirmed by some that velocity, almost to the exclusion of mass, is the operative factor in wounding power. From a theoretical standpoint, velocity can be the dominant determinant of kinetic energy (KE); doubling the mass only doubles the KE, whereas doubling the velocity quadruples the KE. However, from a practical standpoint, doubling the velocity is very difficult to achieve. The M-16 represents only a 10% increase in velocity over the M-14 it replaced. On the other hand, quadrupling the mass is easy. Switch from a .22 to a .44 caliber projectile and you immediately square the mass; then double the length of the projectile so that it flies straighter and you now have an eightfold increase in KE at the same velocity. There are some who mistakenly believe that only the more modern, higher velocity projectiles produce temporary cavitation. The 1870-1890 Vetterli deforming bullet, typical of the military rounds utilized at that time, is depicted in Figure 2. It should be noted that in spite of its relatively low velocity, only 1,357 ft/sec, a very substantial temporary cavity is produced. The formation of a temporary cavity is not a new phenomenon associated with modern high-velocity weapons.
Some maintain that a larger-exit-than-entry wound is evidence of the devastating potential of increases in velocity. While this in fact may be the case (and exit wounds are larger than entry wounds in about 60 percent of the cases), the difference in the size of the wound of entry and exit is not per se directly attributable to velocity since the velocity is greater at the smaller entry wound and lesser at the greater exit wound. The larger exit wound, when present, is caused by projectile yaw, by projectile fragmentation, or as a result of multiple secondary bone fragment projectile. Projectile yaw represents a deviation of the longitudinal axis of the bullet from its line of flight. Rifling within the gun barrel impacts a spin to the bullet, which stabilizes the projectile's flight in air, preventing yaw. The stability imparted by rifling is not enough to prevent yaw in tissues or when the missile passes through foliage or other intermediate objects. Tumbling simply represents yaw that has progressed to a full 180░, at which point the center of mass results in stabilized base forward flight. The point to be borne in mind is that while the high-velocity projectile has the potential for higher energy transfer with subsequent greater tissue disruption, this may not always be the case. Whereas the military surgeon should have some familiarity with wound ballistics and the "worst case" result of high-velocity missile wounds, the surgeon is better advised to concern himself with the individual wound that confronts him rather than with the variable potential of the weapon. On the other hand, wounds of the brain, liver, and heart caused by high-velocity projectiles are catastrophic in nature. The study of wound ballistics attempts to predict and to analyze the damage that will be sustained by the different tissue types when struck by missiles of varying sizes, shapes, weights, and velocities. Missiles that penetrate the human body disrupt, destroy, or contuse tissue, invariably resulting in a contaminated wound. Subsequent triage and treatment decisions are based upon an estimation of the type of wound, the location of the wound, and the amount of tissue disruption. Objective data from the physical examination and appropriate roentgenographic studies of the casualty provide the information necessary to make these decisions.
Approved for public release; Distribution is unlimited. The listing of any non-Federal product in this CD is not an endorsement of the product itself, but simply an acknowledgement of the source. Operational Medicine 2001 Health Care in Military Settings
This web version is provided by The Brookside Associates Medical Education Division. It contains original contents from the official US Navy NAVMED P-5139, but has been reformatted for web access and includes advertising and links that were not present in the original version. This web version has not been approved by the Department of the Navy or the Department of Defense. The presence of any advertising on these pages does not constitute an endorsement of that product or service by either the US Department of Defense or the Brookside Associates. The Brookside Associates is a private organization, not affiliated with the United States Department of Defense. |