|
|
Medical Education Division |
Operational Medicine 2001
GMO Manual
Home · Military Medicine · Sick Call · Basic Exams · Medical Procedures · Lab and X-ray · The Pharmacy · The Library · Equipment · Patient Transport · Medical Force Protection · Operational Safety · Operational Settings · Special Operations · Humanitarian Missions · Instructions/Orders · Other Agencies · Video Gallery · Phone Consultation · Forms · Web Links · Acknowledgements · Help · Feedback
|
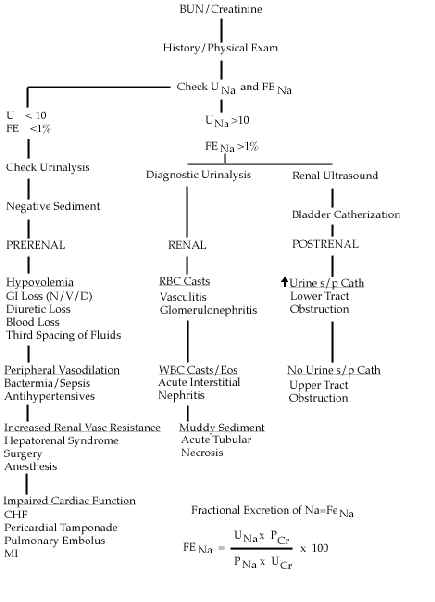
General Medical Officer (GMO) Manual: Clinical Section Acute Renal FailureDepartment of the Navy Acute renal failure (ARF) means sudden reduction of kidney function, leading to bodily retention of nitrogenous wastes. Suspect the diagnosis in the setting of elevated BUN (>20 mg/dl) and serum creatinine (rise of >1 mg/dL/day) with or without oliguria (urine output of <400 mL/day). A wide variety of factors can underlie the development of ARF. For purposes of diagnosis and treatment, these factors are classified as prerenal, postrenal, and intrinsic to the kidneys. ARF may result from decreased effective arterial blood volume (intravascular volume loss, extravascular volume loss, increased vascular capacity, or fluid shifts from intravascular to extravascular spaces), congestive heart failure, or physical obstruction of renal blood flow.
Ureteral obstruction.
Atonic bladder.
Bladder neck obstruction.
Tubulointerstitial.
Glomerulovascular.
A thorough history and physical exam can aid in finding the underlying cause of ARF.
Examination of the Urine in ARF A urinalysis can provide important clues to the etiology of ARF.
Management Measures In ARF
Specific Criteria for Dialysis in ARF
Acute renal failure can arise from a multitude of causes. Differentiation among prerenal, postrenal, and intrinsic causes proves useful for diagnosis, therapy, and prognosis. Patients may present with many or none of the manifestations of either the cause or the effect of renal failure. With few clinical clues, physicians must recognize the common settings in which acute renal failure develops and must order appropriate tests promptly. With advanced renal disease, severe derangements may necessitate urgent intervention by the nephrologist to stabilize the patient.
Approved for public release; Distribution is unlimited. The listing of any non-Federal product in this CD is not an endorsement of the product itself, but simply an acknowledgement of the source. Operational Medicine 2001 Health Care in Military Settings
This web version is provided by The Brookside Associates Medical Education Division. It contains original contents from the official US Navy NAVMED P-5139, but has been reformatted for web access and includes advertising and links that were not present in the original version. This web version has not been approved by the Department of the Navy or the Department of Defense. The presence of any advertising on these pages does not constitute an endorsement of that product or service by either the US Department of Defense or the Brookside Associates. The Brookside Associates is a private organization, not affiliated with the United States Department of Defense. |