Hospital Corpsman Sickcall Screener's Handbook
BUMEDINST 6550:9A
Naval Hospital Great Lakes
1999
Your Command: Student Handout, Laboratory
GAIN ATTENTION: During normal routine the CA will be called upon to order, read, and possibly perform various lab tests.
|
 |
|
KOH Prep
Video
How to do it
training film - 5:00 minutes
Available as Download, CD or DVD
www.brooksidepress.org |
PURPOSE: The purpose of this lesson is to familiarize the student with lab requests, functions of the lab test, and values of the lab results.
INTRODUCE LEARNING OBJECTIVES:
-
TERMINAL LEARNING OBJECTIVE: Given the need to order, read or perform a lab test, the student will be able to do so according to proper procedure.
-
ENABLING LEARNING OBJECTIVES:
-
Be able to select the correct values for lab test by selecting the correct response.
-
Be able to select the correct lab test for different disorders by selecting the correct response.
-
Be able to select the different enzymes and their values by selecting the correct response.
-
The instructor will give this class by lecture and demonstration.
-
This material will be covered on a daily quiz and the final oral exam.
|
 |
|
Operational Medicine CD
Text, images,
videos and manuals
The essential text for military healthcare providers
www.brooksidepress.org |
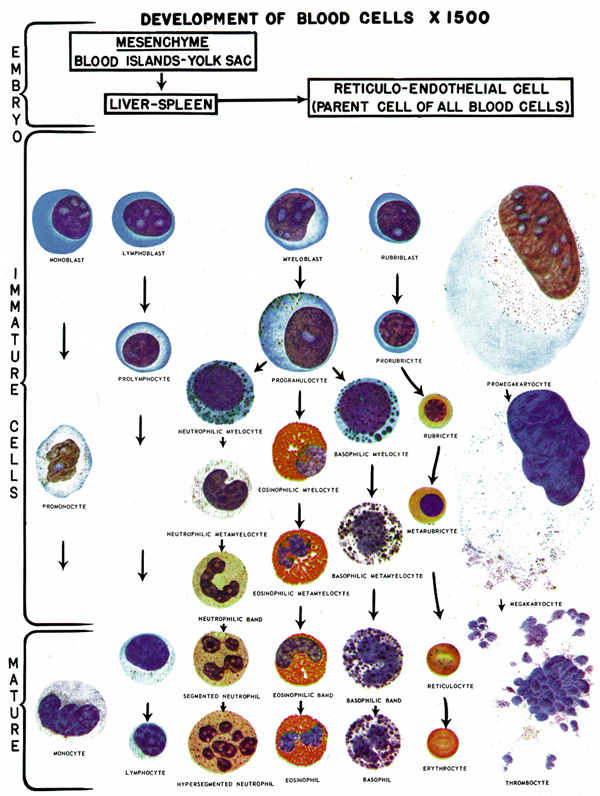
Complete Blood Count (CBC)
-
Red Blood Cells (RBC’s), Erythrocytes
-
RBC’c are the oxygen carrying cells of the blood. The normal range is 5.0 (4.5-6.0) x 106 cells/cc for males and 4.5 (4.0-5.5) x 106 cells/cc for females.
-
Mean Corpuscular volume (MCV) is a measure of the size of RBC’s. Normal is 80-100.
-
An anemia is a condition of decreased oxygen carrying capacity in the blood caused by a decreased number of RBC’s. Anemias are classified according to the size of the RBC’s.
-
Microcytic anemia:(MCV < 80) Found in chronic blood loss, iron deficiency, lead poisoning, chronic infection and in inherited anemias.
-
Normocytic anemia:(MCV 80-100) Found in sudden blood losss, hemolytic anemia, pregnancy, chronic disease, G6PD deficiency and other conditions.
-
Macrocytic anemia:(MCV > 100) Is noted in B12 deficiency, folate deficiency, leukemias, and in liver and thyroid disease.
-
The most common cause of anemia in our population is acute and chronic blood loss and the inherited anemias. All anemias should be referred to a Medical Officer.
-
The term for increased RBC’s is polycythemia, and can be caused by living at high altitudes, vigorous exercise, use of anabolic steroids, a blood condition called polycythemia vera and others.
-
Hematocrit (HCT) is the volume of the RBC’s expressed as a percent of the volume of whole blood. Normal range in males is 45% (45-52%) and in females 40% (36-47%). HCT is determined by placing a drop of blood in a capillary tube and spinning it in a centrifuge. It can also be calculated by automated counter from the relationship HCT = MCV x RBC’s.
-
Hemoglobin (Hgb) is the iron containing pigment of the blood. Normal range in males (14-18%) and in females (12-16%). Its function is to carry oxygen from the lungs to the tissue.
-
Rules of three: When evaluating RBC, Hgb, and HCT remember that:
RBC x 3 = Hgb, and Hgb x 3 = HCT. If the numbers do not follow this rule, i.e. RBC is 5, Hgb is 10 and HCT is 45 then there is a lab error.
-
Keep in mind that lab values may vary from place to place depending on the equipment used.
-
White Blood Cells (WBC’s), Leukocytes
-
WBC’s are the cells involved in fighting infection and in inflammation. The normal range for adults is 4500-11000 cells/mm3. Blacks tend to have lower WBC’s than Whites.
-
The causes of increased WBC’s are many, but included are bacterial infections, acute inflammatory disorders (e.g. rheumatoid arthritis), metabolic disorders (e.g. diabetic acidosis), stress, tissue breakdown (e.g. burns), drugs, toxins, and others.
-
The causes of decreased WBC’s are also many but include some bacterial infections such as influenza, protozoa infections such as malaria, chemical and physical agents such as radiation and others.
-
There are several types of white blood cells which may be distinguished when stained by Wrights Stain on a microscope slide. This is called a differential and is helpful to identify the cause of an abnormal WBC total count.
-
Segmented neutophils are WBC’s that have nuclei that are segmented. They normally comprise 40-60% of the WBC’s in a differential.
-
Band neutrophils are WBC’s that have a band-like or horseshoe shaped nuclei. Normal range is 0-3% of the differential. They are an early form of segmented neutrophils.
-
Lymphocytes are WBC’s with clear sky blue cytoplasm, scanty, with few unevenly distributed granules with a halo around them. Normal range is 10-35%.
-
Monocytes are the largest normal WBC’s. Its color resembles that of a lymphocyte, but its cytoplasm is a muddy grey-blue. Normal range is 4-8%.
-
Eosinophils are characterized by numerous coarse, reddish-orange granules in the cytoplasm which are lighter colored than the nucleus. Normal range is 1-3%.
-
Basophils are characterized by scattered large, dark-blue to purple granules, which are darker than the nucleus. Normal range is 0-1%.
-
The differential is usually written as a series of numbers that add up to 100% in the following order: segmented neutrophils, bands, lymphocytes, monocytes, eosinophils, basophils. Thus a normal differential might be: 55 / 3 / 35 / 5 / 1 / 1. Normal differential might be: 80 / 10 / 9 / 1 / 0 / 0. Notice that the numbers are moving to the left of the series, which is where the term "left shift" comes from when describing differentials. A left shift is viewed as evidence of infection, especially bacterial infection.
-
Platelets
-
Platelets are small, round cells that can be seen on a microscope slide and are important in blood coagulation. The normal range is 200,000-500,000 cells/mm3. There is a tendency to bleed or bruise easily when the platelet count falls to 20,000-50,000 cells/mm3.
Urinalysis (UA)
-
Dipstick test. A number of tests may be performed by dipping a chemical analysis strip into a cup of urine and reading the color coded patches against the references on the strip bottle.
-
Specific gravity is the weight of a liquid compared with an equal volume of water. Water is represented by 1.000. Normal range is 1.010-1.030. A higher concentration is a sign of dehydration.
-
PH is the measure of hydrogen ions in solutions. H2O is neutral and has a PH of 7. Urine is normally acidic with a PH of 5 to 7.
-
Glucose should not be present in normal urine.
-
Ketones should not be present in normal urine.
-
Protein is sometimes present in trace amounts in normal urine.
-
Occult blood should not be present in normal urine. Note: If positive and the microscopic is negative for RBC’s it is generally because of release of myoglobin from muscle breakdown.
-
Urobilinogen is sometimes present in trace amounts in normal urine.
-
Leukocyte Esterase: an enzyme found in neutrophils. Should be negative.
-
Microscopic: seldom done on a routine UA unless the dipstick is positive.
-
Epithelial cells: a few of these cells may be seen in a normal sample, but many epithelial cells may mean the sample is dirty and not collected properly.
-
WBC’s: 1-3 cells per high power field may be seen in normal sample. The presence of WBC’s indicates infections or inflammation involving the urinary tract.
-
RBC’s: 0-2 cells per high power field may be normal prostate hypertrophy, tumors, and other conditions. A common cause of microscopic hematuria in our population is excess exercise, particularly running and humping.
-
Bacteria: rare bacteria may be seen, but many bacteria with WBC’s indicates infection.
-
Casts: 0-1 hyalin per cast per lowe power field may be normal, but other casts are abnormal nad indicate kidney disease.
-
Crystals: may also be seen in normal urine.
-
Collecting and Processing
-
Routine urinalysis requires a random sample. An early morning sample is preferred: a first void when evaluating for sexually transmitted disease: a midstream when evaluating other conditions.
-
A specimen should be analyzed within two hours of collection. If a specimen is left standing it will become alkalinized, and not suitable for culture, RBC’s if present will decompose and urine casts if present will disintegrate.
-
When a 24 hour urine collection is needed, patients should be told to urinate in the morning in the toilet first, then for the rest of the day collect the urine in the container. The next morning they should urinate into the container and bring the sample to the lab. Normal volume is 1000-1600 cc/day.
Chemistry Test
-
Chemistry tests are commonly ordered as groups of tests such as SMA-6, SMA-12, liver function tests (LFT’s), and chemistry panel. The tests that are actually included in these groups varies from lab to lab.
-
Electrolytes
-
Sodium is an important ion that acts to preserve a balance between other ions such as calcium and potassium to maintain normal heart actions and equilibrium of the body. Normal range 136-145 mmol/L.
-
Potassium is essential for normal excitability of muscle tissue, especially heart muscle. It also plays a role in the condition of nerve impulses. Normal range 3.5-5.0 mmol/L.
-
Calcium is used by the body for bone growth, blood coagulaiton, and nerve, mucsle and heart function. Normal is 2.2-2.6 mmol/L. (9-10.5 mg/dL)
-
Chloride is the predominant negative ion in plasma. Normal range 98-106 mmol/L.
-
CO2 is the sum of the concentration of bicarbonate and carbonic acid in plasma. Normal range 21-30 mmol/L.
-
Phosphate is a negative ion involved in bone metabolism and energy production. Normal range is 1.0-1.4 mmol/L. (3-4.5 mg/dL)
-
Electrolytes are ordered for a wide variety of reasons including kidney disease, dehydration, GI disease, heart disease, metabolic disease, etc.
-
Renal Function Tests
-
Blood Urea Nitrogen (BUN) is a measure of nirtogen in the blood as urea, a breadkown product of proteins. Normal range 3.6-7.1 mmol/L.
(10-20 mg/dL)
-
Creatinine is the end product of creatine metabolism and is excreted by the kidney. Normal range < 133 mmol/L. (<1.5 mg/dL)
-
Liver Function Test
-
Alkaline phosphates is an enzyme found in liver, bone, intestine and placenta that is increased with liver disease. Normal range is 30-125 mu/ml.
-
SGOT (AST), Serum Glutamic-oxaloacetic Transaminase, is an exzyme found in many tissues, but in highest concentration in the liver and heart. Injury of either causes release of the enzyme into the blood. Normal is less than 40 units/liter.
-
SGPT (ALT), Serum Glutamic-pyruvic Transaminase is found more specifically in the liver. Normal is less than 40 units/liter.
-
Bilirubin is a yellowish pigment that is a breakdown product of hemoglobin and is Processed and excreted by the liver. Increased blood breakdown or liver disease or obstruction will cause bilirubin to rise above normal 0.3 to 1.0 mg/dL. When bilirubin reaches between 2 to 4 the sclera and the skin become tinted yellow.
-
Others
-
Glucose is used as the primary source of energy for the body. Normal range is 65-120 mg/dl.
-
Total protein is the sum of the circulating proteins in the serum and is difficult to interpret without knowledge of the individual fractions. Normal range 6.0 to 8.5 g/dl.
-
Albumin is a protein made in the liver. It is decreased in liver, kidney, GI, and chronic disease and malnutrition. It is increased in dehydration. Normal range 3.5 to 5.0 g/dl.
-
Globulin is the other major protein in the serum. Globin composes most of the fraction of total protein that is not albumin.
-
Uric Acid is an end product of uricotelic metabolism. Normal range is 2.5 to 8.0 mg/dl in males and 1.5 to 6.0 mg/dl in females.
-
CPK, or creatine phosphokinase, is an enzyme present in skeletal and heart muscle, and is increased in muscle breakdown and heart attacks. Normal is 25 to 235 u/liter.
-
LDH, lactate dehydrogenase, is an enzyme present in various tissues and serum which is important in the exidation of lactate. Normal range is 100 - 225 u/liter.
-
Lipids
-
Cholesterol is a fatty substance in the blood. High levels of cholesterol are associated with coronary atherosclerotic disease and varies with age. A value of cholesterol greater than 200 mg/dl for any age group is abnormal.
-
Triglycerides are the other magor fatty substance in the blood, and should be measured on a patient who has fasted for 12-24 hrs. He/she may drink all the water they wish. Normal is 10-140 mm/dl.
Cultures (C&S)
-
Urine culture: Patients should be given a sterile urine cup and instructed as follows:
-
First morning specimen: wash hands thoroughly, wash penis or vulva with downward strokes, start to urinate into the toilet, stop and position container and take sample, screw on cap without touching inside rim, take to lab immediately. A positive culture grows bacteria CFU > 104/cc of urine.
-
Gonorrhea culture: Specimen may be obtained from the cervix, vagina, urethra, rectum, throat or joint fluid. Specimens are cultured on Thayer-Martin medium.
-
Samples from the urethra in males are obtained as follows: do not collect until at lest one hour after last urination, collect discharge directly or from discharge obtained by "milking" the urethra, if no discharge is abailable, insert an unmoistened thin swab into the urethra approximately 2 cm and gently rotate it.
-
Another approach to obtaining a specimen in an asymptomatic male, which is not embarrassing to the patient, is as follows: collect a first void (not midstream) urine specimen and send to the lab for GC gram stain and culture of sediment.
-
Throat culture: The most common bacterial cause of pharyngitis is group A beta hemolytic streptococci. Patients with pharyngitis are at an increase risk of acute rheumatic fever and post streptococcal glomerulonephritis.
-
Obtain a specimen before starting antibiotics.
-
Depress the tongue to expose the pharynx. Use a culturette or sterile cotton swab. Rub the swab vigorously over the posterior pharynx and tonsils, avoiding the tongue, uvula and buccal mucosa.
-
Stool cultures: Should be obtained in any patient with diarrhea lasting longer than two (2) days, diarrhea with high fever, bloody or mucous containing diarrhea or diarrhea in moderately to severely ill patients. Rectal swabs, culturettes or fresh stool samples should not be refrigerated and should be delivered to the lab in less than four hours.
-
Wound and abcess cultures: Should be obtained from the edges of wounds and abcesses. The center of abcesses are generally sterile.
-
Blood cultures: Usually obtained in very ill patients with fever of unknown origin and in other clinical situations.
-
Sputum culture: Should be obtained when the patient suspected of pneumonia has a productive cough. Early morning samples are best, and a gram stain should be ordered on the same sample. A significant number of epithelial cells indicate the sample is probably saliva and not sputum.
KOH Prep
-
A KOH Prep is used for the diagnosis of fungal ingection. Samples should be taken at the edge of the skin lesions and placed on a microscope slide with a couple of drops of KOH. The KOH dissolves all the cells except fungal cells, making them easier to see under the microscope. Fungal elements appear as branching structures looking like bamboo, sometimes with small buds.
FINAL NOTE: Although "normal" values have been quoted above, all normal laboratory values vary from lab to lab.
|
|
Approved for public release;
Distribution is unlimited.
The listing of any non-Federal product in this CD is not an endorsement of the
product itself, but simply an acknowledgement of the source.
Bureau of Medicine and Surgery
Department of the Navy
2300 E Street NW
Washington, D.C
20372-5300 |
Operational Medicine
Health Care in Military Settings
CAPT Michael John Hughey, MC, USNR
NAVMED P-5139
January 1, 2001 |
United States Special Operations
Command
7701 Tampa Point Blvd.
MacDill AFB, Florida
33621-5323 |
*This web version is provided by
The Brookside Associates Medical Education Division. It contains
original contents from the official US Navy NAVMED P-5139, but has been
reformatted for web access and includes advertising and links that were not
present in the original version. This web version has not been approved by the
Department of the Navy or the Department of Defense. The presence of any
advertising on these pages does not constitute an endorsement of that product or
service by either the US Department of Defense or the Brookside Associates. The
Brookside Associates is a private organization, not affiliated with the United
States Department of Defense.
Contact Us · · Other
Brookside Products
|
|
Operational Medicine 2001
Contents
|

|
 |
|
FMST Student Manual Multimedia CD
30 Operational Medicine Textbooks/Manuals
30 Operational Medicine Videos
"Just in Time" Initial and Refresher Training
Durable Field-Deployable Storage Case |
|

