|
5-1. INTRODUCTION
The body was designed for motion. Regular exercise
contributes to a healthy body; therefore immobility has a negative effect. A
joint that has not been moved sufficiently can begin to stiffen within 24
hours and will eventually become inflexible. With longer periods of joint
immobility, the tendons and muscles can be affected as well.
Most people move and exercise their joints through the
normal activities of daily living. When any joint cannot be moved in this
way, the patient or nurse must move it at regular intervals to maintain
muscle tone and joint mobility.
Range of motion (ROM) exercises are ones in which a nurse or
patient move each joint through as full a range as is possible without
causing pain. The effect of both regular exercise and immobility on major
body systems are discussed in this
lesson.
5-2. THE EFFECTS OF
IMMOBILITY
Cardiovascular System.
-
Venous stasis caused by prolonged inactivity that
restricts or slows venous circulation. Muscular activity, especially in
the legs, helps move blood toward the central circulatory system.
-
Increased cardiac workload due to increased viscosity from
dehydration and decreased venous return. The heart works more when the
body is resting, probably because there is less resistance offered by the
blood vessels and because there is a change in the distribution of blood
in the immobile person. The result is that the heart rate, cardiac output,
and stroke volume increase.
-
Thrombus and embolus formation caused by slow flowing
blood, which may begin clotting within hours, and an increased rate in the
coagulation of blood. During periods of immobility, calcium leaves bones
and enters the blood, where it has an influence on blood coagulation.
-
Orthostatic hypotension probably due to a decrease in the
neurovascular reflexes, which normally causes vasoconstriction, and to a
loss of muscle tone. The result is that blood pools and does not squeeze
from veins in the lower part of the body to the central circulatory
system. The immobile person is more susceptible to developing orthostatic
hypotension. The person tends to feel weak and faint when the condition
occurs.
Respiratory System.
-
Hypostatic pneumonia. The depth and rate of respirations
and the movement of secretions in the respiratory tract is decreased when
a person is immobile .
The pooling secretions and congestion predispose to
respiratory tract infections. Signs and symptoms include:
-
Increased temperature.
-
Thick copious secretions.
-
Cough.
-
Increased pulse.
-
Confusion, irritability, or disorientation.
-
Sharp chest pain.
-
Dyspnea.
Atelectasis. When areas of lung tissue are not used over a
period of time, incomplete expansion or collapse of lung tissue may occur.
Impaired coughing. Impairment of coughing mechanism may be
due to the patient's position in bed decreasing chest cage expansion.
Musculoskeletal System.
-
Muscle atrophy. Disuse leads to decreased muscle size,
tone, and strength.
-
Contracture. Decreased joint movement leads to permanent
shortening of muscle tissue, resistant to stretching. The strong flexor
muscles pull tight, causing a contraction of the extremity or a permanent
position of flexion.
-
Ankylosis. Consolidation and immobility of a joint in a
particular position due to contracture.
-
Osteoporosis. Lack of stress on the bone causes an
increase in calcium absorption, weakening the bone.
Nervous System.
-
Altered sensation caused by prolonged pressure and
continual stimulation of nerves. Usually pain is felt at first and then
sensation is altered, and the patient no longer senses the pain.
-
Peripheral nerve palsy.
Gastrointestinal System.
-
Disturbance in appetite caused by the slowing of
gastrointestinal tract, secondary immobility, and decreased activity
resulting in anorexia.
-
Altered digestion and utilization of nutrients resulting
in constipation.
-
Altered protein metabolism.
Integumentary System.
Risk of skin breakdown, which leads to necrosis and ulceration of tissues, especially on bony areas.
Urinary System.
-
Renal calculi (kidney stones) caused by stagnation of
urine in the renal pelvis and the high levels of urinary calcium.
-
Urinary tract infections caused by urinary stasis that
favors the growth of bacteria.
-
Decreased bladder muscle tone resulting in urinary
retention.
Metabolism.
-
Increased risk of electrolyte imbalance. An absence of
weight on the skeleton and immobility causes protein to be broken down
faster than it is made, resulting in a negative nitrogen balance.
-
Decreased metabolic rate.
-
Altered exchange of nutrients and gases.
Psychosocial Functioning.
-
Decrease in self-concept and increase in sense of
powerlessness due to inability to move purposefully and dependence on
someone for assistance with simple self-care activities.
-
Body image distortions (depends on diagnosis).
-
Decrease in sensory stimulation due to lack of activity,
and altered sleep-wake pattern.
-
Increased risk of depression, which may cause the patient
to become apathetic, possibly because of decreased sensory stimulation; or
the patient may exhibit altered thought processes.
-
Decreased social interaction.
5-3.
THE PURPOSES OF
EXERCISE FOR THE IMMOBILE PATIENT
-
To maintain joint mobility is done by putting each of the
patient's joints through all possible movements to increase and/or
maintain movement in each joint.
-
To prevent contracture, atony (insufficient muscular
tone), and atrophy of muscles.
-
To stimulate circulation, preventing thrombus and embolus
formation.
-
To improve coordination.
-
To increase tolerance for more activity.
-
To maintain and build muscle strength .
5-4. TYPES OF EXERCISES
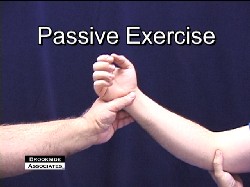
-
Passive.
These exercises are carried out by the nurse, without
assistance from the patient. Passive exercises will not preserve muscle
mass or bone mineralization because there is no voluntary contraction,
lengthening of muscle, or tension on bones.
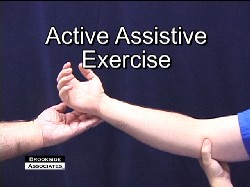
-
Active Assistive.
These exercises are performed by the patient with assistance from the
nurse. Active assistive exercises encourage normal muscle function while
the nurse supports the distal joint.
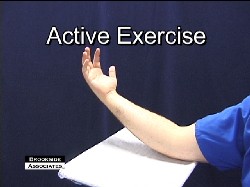
-
Active.
Active exercises are performed by the patient, without assistance, to
increase muscle strength.
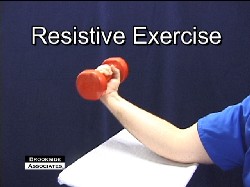
-
Resistive.
These are active exercises performed by the patient by pulling or pushing
against an opposing force.
-
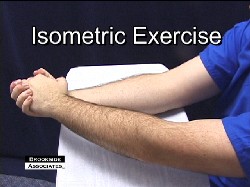
Isometric.
These exercises are performed by the patient by contracting and relaxing
muscles while keeping the part in a fixed position. Isometric exercises
are done to maintain muscle strength when a joint is immobilized. Full
patient cooperation is required.
The Brookside
Associates Medical Education Division is dedicated to the development and
dissemination of medical information that may be useful to medical professionals
and those in training to become medical professionals. This website is
privately-held and not connected to any governmental agency. The views expressed
here are those of the authors, and unless otherwise noted, do not necessarily
reflect the views of the Brookside Associates, Ltd., any governmental or private
organizations. All writings, discussions, and publications on this website are
unclassified.
© 2007 Medical Education
Division, Brookside Associates, Ltd. All rights reserved
Other
Brookside Products
Contact Us
Advertise on this Site
|
|