Ectopic Pregnancy
Incidence · Ectopics
of Special Significance · Symptoms
· Physical
Findings · Laboratory
· Ultrasound
· Culdocentesis
· D&C
· Laparoscopy
· Laparotomy
· Medical Management
· Expectant Management
· Followup
· Military
Settings
Ectopic pregnancy means the pregnancy is not growing in its normal
location inside the uterus. Instead, it is growing elsewhere. 97% of the
time, the ectopic pregnancy is located in the fallopian tube (tubal
ectopic pregnancy) and the rest are found in the ovary, abdomen, cervix
or other nearby structure.
Unruptured tubal ectopic pregnancy |
Incidence
The incidence of ectopic pregnancy varies with the population but is
about one in every hundred pregnancies. The incidence is higher among
women with previous tubal disease, tubal surgery, previous ectopic
pregnancy, assisted reproduction, and current IUD users. Many very early
ectopic pregnancies resolve spontaneously, so if you aggressively search
for them early in pregnancy, you will find more of them.
Ectopic
Pregnancies of Special Clinical Interest
Certain types of ectopic pregnancy carry special significance. Among
these are:
-
Implantation in the distal half of the fallopian tube. This
represents the vast majority of all ectopics and is the type most
likely to resolve spontaneously through "tubal abortion." The closer
the ectopic is to the fimbriated end, the more likely it will be to
outgrow its blood supply and be expelled out the end of the tube.
-
Isthmic ectopic. The isthmus is the narrowest portion of the tube,
least distensible, and ectopics that grow here are more likely to
rupture, and to rupture early in the course of the pregnancy.
-
Cornual ectopic. These ectopics grow in the portion of the tube
that passes through the uterine cornua. These tend to rupture early
and violently, with massive abdominal hemorrhage. Many of the
fatalities due to ectopic pregnancy are from cornual pregnancies.
Symptoms
For women without rupture, there may be no symptoms, other than the
usual symptoms of pregnancy (fatigue, breast tenderness, amenorrhea).
With rupture and intra-abdominal bleeding, the following symptoms may be
seen, depending on the extent of bleeding:
Physical Findings
In the case of unruptured ectopic pregnancies in the fallopian tube,
there may be no unusual physical findings. The uterus can be enlarged
appropriately, no masses found, and no tenderness in the pelvis. Some
patients, however, may show some of these findings:
-
Pelvic mass (either from the enlarged ectopic, or from the corpus
luteum cyst that accompanies many early pregnancies of all types)
-
Pelvic tenderness, localized or geeralized
-
Abdominal distension
-
Hypotension, tachycardia, tachypnea
Laboratory
The pregnancy test is positive.
-
Serial Quantitative HCG levels often are low and do not show the normal doubling every 2 days.
However, some (10-15%) ectopic pregnancies do show a normal rise, and
some (10-15%) normal pregnancies don't show the normal doubling rate.
-
Progesterone levels are
sometimes very low (<5). Levels greater than 25 are usually seen with
normal intrauterine pregnancies, but this is a generalization.
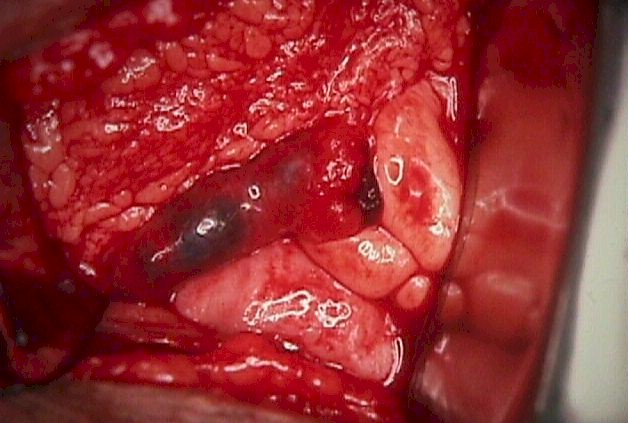
Unruptured cornual ectopic pregnancy |
Ultrasound
As the resolution of ultrasound has improved over the years, so has
its ability to find ectopic pregnancies. It still remains true, however,
that ultrasound is at its best in defining the presence of normal,
intrauterine pregnancies. Some of the criteria for defining an ectopic
pregnancy with ultrasound include:
-
Visualization of a gestational sac, fetal pole and fetal heartbeat
outside of the uterus. This is an uncommon finding with ectopic
pregnancies.
-
Absence of an identifiable intrauterine pregnancy when the
quantitative HCG suggests
it should be visible. The "discriminatory zone" is the level of HCG, above which a normal
IUP is normally seen. The discriminatory zone varies from setting to
setting and depends on both the skills of the operator, the resolution
of the equipment, and the imaging technique (abdominal vs vaginal).
Discriminatory zones range from 1,000 to 2,000 or more, depending on
the clinical setting.
-
Free fluid in the abdomen if there is any significant internal
bleeding.
Ultrasound can be misleading at times. Occasionally, "intrauterine"
pregnancies are identified that are, in fact, ectopic pregnancies with
sufficient inflammatory reaction and bleeding around them to make it
appear that they are surrounded by normal uterine muscle. In some other
cases, an "intrauterine" pregnancy is identified that is, in fact, a
"gestational pseudosac" within the uterus. This pseudosac is a response
by the endometrium to the hormones of pregnancy and can mimic the
appearance of an intrauterine pregnancy.
Culdocentesis
Culdocentesis may be performed to gain additional information. A needle
is inserted through the vaginal wall into the posterior culdesac. These
findings are possible:
-
A dry tap is inconclusive
-
A few cc's of clear fluid (peritoneal fluid) rules out a ruptured
ectopic, but neither rules out nor in an unruptured ectopic.
-
Slightly bloody fluid (hct <15)
is inconclusive. This could be from a traumatic tap, or early, mild
bleeding from an ectopic.
-
Moderately bloody fluid (hct
>15) indicates hemoperitoneum consistent with ruptured ectopic,
but is non-specific and any internal bleeding (hemorrhagic ovarian
cyst) can give this result.
-
Bright red, clotting blood usually indicates a traumatic tap or
aspiration of blood from a vessel.
D&C
Dilatation and curettage is sometimes done in the presence of a clearly
abnormal HCG pattern,
combined with abnormal ultrasound findings, to confirm or rule out
ectopic pregnancy. If the D&C specimen shows chorionic villi, then the
pregnancy was intrauterine. If no chorionic villi are found, then
ectopic pregnancy is often presumed to be present.

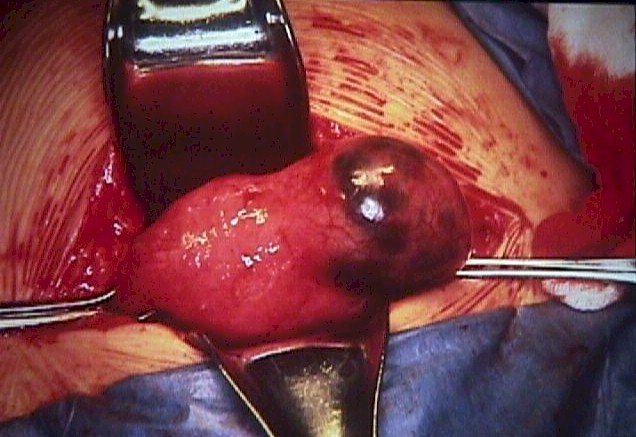
Salpingectomy with ectopic pregnancy
removed from the tube |
Laparoscopy
Laparoscopy is a very effective method to diagnose ectopic pregnancy.
Unfortunately, it is invasive, carrying its own risks, and may miss very
early ectopic pregnancies that have not grown large enough to be
appreciated by the operator.
When ectopic pregnancies are found with
laparoscopy, it is often possible to remove them surgically at the same
time. An incision is made over the antimesenteric border of the tube and
the ectopic is teased out. This can be facilitated by the injection of
pitressin into the tube, causing the muscularis layer to contract,
expelling the ectopic and controlling bleeding. Bleeding usually either
stops or is controlled with judicious use of cautery.
Not all cases of ectopic pregnancy lend themselves to
laparoscopic surgery. The larger the ectopic, the more difficult and
dangerous is the laparoscopic surgery. The more bleeding that is
present, the more difficult and dangerous is the laparoscopic surgery.
Cornual and some isthmic ectopic pregnancies usually will need
laparotomy to effectively control bleeding from the uterine side.
Laparotomy
At times, laparotomy is the best choice for dealing with an ectopic
pregnancy, particularly if the patient is bleeding heavily or is
clinically unstable.
In these cases, the priority is stopping the
blood loss. The fastest and simplest way to do that is to clamp across
the blood supply of the ectopic, remove it, and sew up the cut edges.
This is known as a salpingectomy or partial salpingectomy, depending on
the extent.
In the past, great effort was made (and considerable risk taken) to
preserve childbearing potential by conserving and repairing the
fallopian tube. Given the advanced state of assisted reproductive
technology, such risks are only infrequently warranted today. The
long-term natural fertility of a woman experiencing an ectopic pregnancy
is about the same (about 50%), whether you remove the entire affected
tube or try to repair it. In the event of subsequent infertility, egg
retrieval, in-vitro fertilization and embryo transfer can usually
leap-frog over the need for functional fallopian tubes, so immediate
surgical safety and speedy recovery are usually the priorities.
Medical Management
Methotrexate is a folate antagonist originally used to treat
trophoblastic disease. It can be an effective treatment for ectopic
pregnancy.
At least half of these patients will have significant abdominal pain,
but the treatment will be successful in about 90% of cases in resolving
the ectopic pregnancy without resorting to surgery. Some of these
patients will still need surgery, either because of persistent or severe
pain, hemorrhage, or failure of the HCG to resolve completely.
Recovery using this method may require up to several months.
Not everyone with an ectopic pregnancy is a good candidate for this
treatment. It works best when:
-
The patient is compliant
-
The patient prefers to avoid surgery (but with the possibility of
even longer recovery from the medical treatment)
-
There is desire for future childbearing
-
The patient is hemodynamically stable
-
The ectopic pregnancy is <3.5 cm in diameter
-
There is no observable fetal cardiac activity
-
There is no evidence of rupture
-
HCG levels are
<15,000
-
There is no hepatic, renal, WBC or platelet dysfunction
 Expectant Management Expectant Management
Not all cases of ectopic pregnancy require surgical or medical
treatment. For many ectopic pregnancies, their natural history will be
to stop growing, detach and be expelled out the end of the fallopian
tube, clinically disappearing.
Expectant management seems to work best
when there is a plateau or falling levels of HCG , and the initial HCG is <1,000, in
asymptomatic women. In such cases, successful spontaneous resolution can
be expected in 75 to 90% of cases. Some of these will ultimately require
methotrexate or surgery to resolve. Expectant management can be
considered in other cases, but the success rate will be less. The
overall successful resolution without surgery or methotrexate for
ectopic pregnancies managed expectantly with initial HCG of <2000 is 60%.
Subsequent fertility has been shown to be about the same, regardless
of whether the ectopic is managed expectantly, with methotrexate, or
surgically.
Followup
It is important that no viable trophoblastic tissue remain following
treatment for ectopic pregnancy. For this reason, followup HCG levels are often drawn
serially to demonstrate complete resolution of the ectopic.
Rh
sensitization can occur following ectopic pregnancy treatment and Rh
immune globulin is administered to Rh negative women to prevent such an
event.
Military Settings
In advanced military settings, surgery may not be immediately available for
women with ectopic pregnancies. In such cases, supportive treatment including IV
fluids, MAST suits, oxygen, bedrest and transfusion as needed can often be
effective management of these patients.
|

