|
|
||||||||
Swollen Neck NodesHistory Everyone has lymph nodes; they act as filters of the blood and lymph. When lymph nodes swell, it is in reaction to something; this is called lymphadenopathy. Lymphadenopathy may be a reaction to an infection, or something noninfectious (such as a lymphoma).
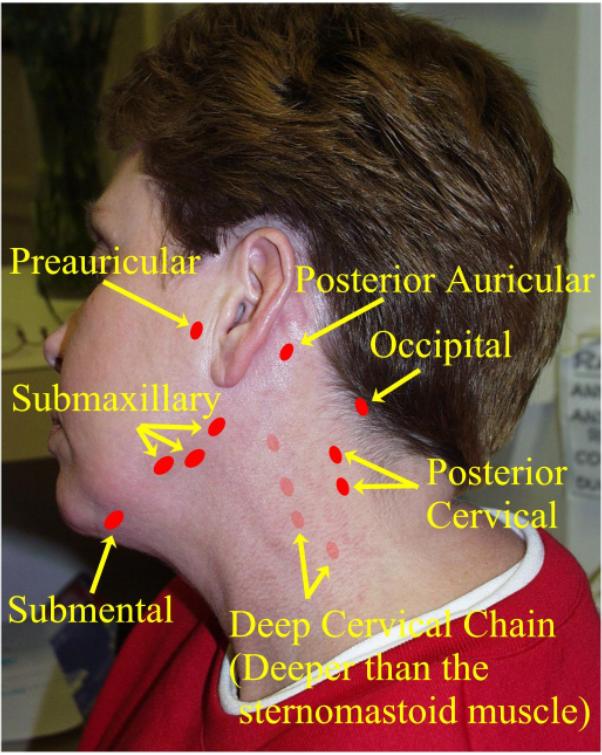
Neck nodes are referred to as “cervical nodes.” Anterior cervical lymphadenopathy is common. Posterior cervical lymphadenopathy (around the trapezius muscle) is unusual, and should suggest either a viral infection (mononucleosis, CMV, or HIV) or a tumor.
Physical Exam
Laboratory Tests
Medications An empiric trial of penicillin may be warranted (provided the patient is not penicillin allergic), especially if there is no way to confirm or exclude the diagnosis of “strep throat.” Patients with mononucleosis almost always develop a rash if they are placed on ampicillin; this rash can be diagnostic of mononucleosis, and should not be confused with a penicillin-rash. Rarely, corticosteroids are useful in mono. Medevac Some of these patients may be very ill. Fever, prostration, dysphagia, and odynophagia can all lead to dehydration. If the patient is unable to swallow, attempt IV fluids. Monitor the blood pressure, or, if no sphygmomanometer is available, the pulse (and its quality) are important. This section provided by CDR Wesley Emmons, MC, USN, Head of Infectious Diseases, Naval Medical Center Portsmouth
Home · Military Medicine · Sick Call · Basic Exams · Medical Procedures · Lab and X-ray · The Pharmacy · The Library · Equipment · Patient Transport · Medical Force Protection · Operational Safety · Operational Settings · Special Operations · Humanitarian Missions · Instructions/Orders · Other Agencies · Video Gallery · Forms · Web Links · Acknowledgements · Help · Feedback Approved for public release; Distribution is unlimited.
*This web version is provided by The Brookside Associates, LLC. It contains original contents from the official US Navy NAVMED P-5139, but has been reformatted for web access and includes advertising and links that were not present in the original version. The medical information presented was reviewed and felt to be accurate in 2001. Medical knowledge and practice methods may have changed since that time. Some links may no longer be active. This web version has not been approved by the Department of the Navy or the Department of Defense. The presence of any advertising on these pages does not constitute an endorsement of that product or service by either the US Department of Defense or the Brookside Associates. The Brookside Associates is a private organization, not affiliated with the United States Department of Defense. © 2015, Brookside Associates, LLC. All rights reserved
|
||||||||