|
|
|||||
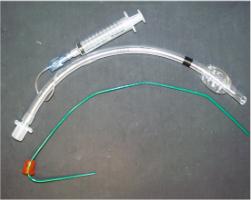
Endotracheal IntubationIdeally,
the patient should be hyperventilated with 100% oxygen for several minutes
prior to intubation.
Assemble
and test equipment while patient is being ventilated:
Lubricate
distal end of tube with water soluble lubricant.
Assistant
holds pt's head, performs Sellick's maneuver and counts slowly to 30.
Intubator
takes a breath and holds it, then directly visualizes cords with
laryngoscope.
If
unable to visualize chords within 30 seconds, or when the intubator has to
take a breath, then remove the laryngoscope
and ventilate the patient for 1 minute. Repeat attempt to visualize the
cords.
When
chords are visualized, advance tube to a depth of 5cm beyond cords.
Inflate cuff and ventilate. Check
the tube placement by listening over the stomach and both lung fields.
Re-position the tube or remove as necessary. Do not release
Sellick’s maneuver until proper position of the tube is confirmed and
the cuff is inflated.
Secure
the tube with adhesive tape once proper placement is confirmed.
Re-confirm position of tube by listening to the lungs every time the patient is moved.
Home · Military Medicine · Sick Call · Basic Exams · Medical Procedures · Lab and X-ray · The Pharmacy · The Library · Equipment · Patient Transport · Medical Force Protection · Operational Safety · Operational Settings · Special Operations · Humanitarian Missions · Instructions/Orders · Other Agencies · Video Gallery · Forms · Web Links · Acknowledgements · Help · Feedback Approved for public release; Distribution is unlimited.
*This web version is provided by The Brookside Associates, LLC. It contains original contents from the official US Navy NAVMED P-5139, but has been reformatted for web access and includes advertising and links that were not present in the original version. The medical information presented was reviewed and felt to be accurate in 2001. Medical knowledge and practice methods may have changed since that time. Some links may no longer be active. This web version has not been approved by the Department of the Navy or the Department of Defense. The presence of any advertising on these pages does not constitute an endorsement of that product or service by either the US Department of Defense or the Brookside Associates. The Brookside Associates is a private organization, not affiliated with the United States Department of Defense.
© 2015, Brookside Associates, LLC. All rights reserved
|
|
||||