|
|
|||||
Debride a WoundFollowing injury from a high velocity projectile, soft tissue wounds will usually need debridement. This means removal of dead or dying tissue, foreign bodies (metal or bone fragments), and other contaminants (pieces of wood, clothing, skin, hair or equipment) from the wound. This debridement is very important:
Four factors are important for a successful debridement:
Normally, skin incisions for debridement in the arms and legs are made longitudinally (parallel to the long bones). Starting at the wound, use a scalpel to incise the skin , extending it far enough to obtain good exposure of the injured tissues. Then make another skin incision, in the opposite direction, again obtaining good exposure. Try not to incise any deeper than the skin to avoid injuring healthy tissue underneath the incision. If the wound or your incisions involves a joint, it is best to obtain consultation (if available) as some incisions over the joints are better than others. Watch a video showing wound debridement Don't put your fingers in the wound. There may
be razor sharp metal or glass fragments that can cut you.
After you are through the skin, most surgeons start using curved scissors. Inserting the closed scissors into the wound tract will help identify the direction you will need to follow to expose devitalized tissues. Skin is normally very well vascularized and little,
if any skin will need to be removed. Shreds of skin can be excised, as
well as any crushed, obviously necrotic skin.
Use scissors and tissue forceps (rat-toothed forceps
or pickups with teeth) to undermine and then cut the subcutaneous tissues
down to the peri-muscular fascia. Try to develop each layer, one at a
time, as this will help prevent unnecessary injury and will help you
maintain your orientation, despite the tissue destruction of the wound.
Undermine the fascia with scissors, and then incise
it. The fascia will need to be generously incised in order to expose the
underlying tissue damage. One old expression is: "The Fascia You
Should Slash(ia)." If any fascia is necrotic, excise it and discard
it.
As you work your way down through the wound, any
loose foreign bodies should be removed, using forceps to avoid injuring
your fingers. Irrigation fluid (such as normal saline or lactated Ringer's
solution) is very helpful in dislodging clots and other foreign material.
It can be dripped in under pressure from an IV bag, pulsed into the wound
using a syringe, or simply poured in periodically. Gauze sponges help keep
the surgical field clear for you to see.
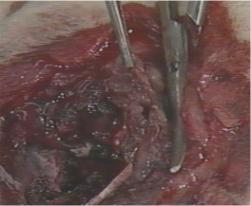
Once through the fascia, you will be able to visualize the underlying muscles. Devitalized muscle is characterized by:
These are sometimes described as the "Four C's"
Devitalized muscle must be removed. Some tissues can
get by for a while with little or no blood supply. Tendons and nerves, if
lying adjacent to other normal tissues, can absorb enough oxygen to
survive. Muscles, however, can't do that. They have a relatively high
metabolic rate and if deprived of oxygen, will die fairly quickly.
Pick up a small piece of devitalized muscle and
excise it with the curved scissors. After it is removed, look at the cut
muscle edge. If it is oozing bright red blood, you have probably excised
enough muscle in that area and you can move to the next area. If the base
is not oozing, it means that you still haven't reached healthy muscle and
you you generally will need to take more out.
The goal is to remove all dead muscle without taking
out very much healthy muscle.
After completing the superficial soft tissue
debridement, then move to the deeper structures and continue debriding.
You may need to debride through the opposite side of
the wound in order to complete the procedure.
Most oozing will simply stop on its' own or with
gentle direct pressure. Larger bleeders may need to be individually
identified, clamped with a fine hemostat, and ligated. Try to clamp just
the bleeding point, and not the surrounding tissues. Use a fine ligature
(thread) to minimize the amount of foreign material left in the wound.
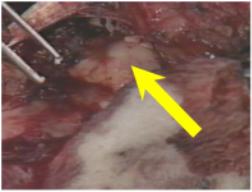
If you encounter white or yellow fat in the wound,
that is a sign that nerve structures are nearby. Nerves are always
well-padded, so observation of fat should serve as a warning that says,
"Watch out. If you cut here, you may cut a nerve." If the
fat is intact, you ordinarily should leave it alone. Fat doesn't require
much oxygen or blood supply and incising it will only set the patient up
for nerve injury.
If at all possible, try not to disrupt nerves or
large blood vessels. The goal is to not just to avoid infection in the
traumatized limb, but to also end up with a functional limb.
After all devitalized tissue is removed, the wound is
loosely packed with gauze, and covered with a loose gauze dressing, The wound is almost never closed immediately,
but left for re-exploration several days later. Closure may be done then,
or even later, via secondary closure, granulation or skin grafting. A
wound that requires debridement is not likely to be a good candidate for
primary closure.
Thus, the basic principles of wound debridement are:
This section was developed from A1701-89-0142 "JMRTC-Surgical Training. Advanced Trauma Life Support. Wound Debridement" with LTC Randolf Copeland, MC, USA, Health Sciences Media Division, US Army Medical Department C&S, Fort Sam Houston, Texas.
Home · Military Medicine · Sick Call · Basic Exams · Medical Procedures · Lab and X-ray · The Pharmacy · The Library · Equipment · Patient Transport · Medical Force Protection · Operational Safety · Operational Settings · Special Operations · Humanitarian Missions · Instructions/Orders · Other Agencies · Video Gallery · Forms · Web Links · Acknowledgements · Help · Feedback Approved for public release; Distribution is unlimited.
*This web version is provided by The Brookside Associates, LLC. It contains original contents from the official US Navy NAVMED P-5139, but has been reformatted for web access and includes advertising and links that were not present in the original version. The medical information presented was reviewed and felt to be accurate in 2001. Medical knowledge and practice methods may have changed since that time. Some links may no longer be active. This web version has not been approved by the Department of the Navy or the Department of Defense. The presence of any advertising on these pages does not constitute an endorsement of that product or service by either the US Department of Defense or the Brookside Associates. The Brookside Associates is a private organization, not affiliated with the United States Department of Defense.
© 2015, Brookside Associates, LLC. All rights reserved
|
|
||||