Breast Problems
Breast Development
Note to readers from
the Brookside Associates:
Although this page faithfully
reproduces the original Operational Medicine 2001, there is a
better (updated, with pictures) version of it in
Military Obstetrics & Gynecology. |
At puberty, the female breast develops, under the influence of estrogen, progesterone,
growth hormone, prolactin, insulin and probably thyroid hormone, parathyroid hormone and
cortisol. This complex process typically begins between ages 8 to 14 and spans about 4
years.
The breast contains mostly fat tissue, connective tissue, and glands that following
pregnancy, will produce milk. The milk is collected in the ducts and transported to 15-25
openings through the nipple.
 During the menstrual cycle, the breast is smallest on days 4-7, and then begins to
enlarge, under the influence of estrogen and later progesterone and prolactin. During the menstrual cycle, the breast is smallest on days 4-7, and then begins to
enlarge, under the influence of estrogen and later progesterone and prolactin.
Maximum breast size occurs just prior to the onset of menses.
The breast is not round, but has a "tail" of breast tissue extending up into
the axilla (or armpit).
This is clinically significant because abnormalities can arise there just as they can
in other areas of the breast. During breast examinations, this area should be palpated.
The breast is divided into quadrants to better describe and compare clinical findings.
The upper outer quadrant is the area of greatest mass of breast tissue. It is also the
area in which about half of all breast cancers will develop.
Breast Examination
A breast examination consists of inspection and palpation of the breasts to identify
abnormalities. Some breast examinations are focused on specific issues while others are
more general. Although there are many good ways to examine the breasts, one of them
will be presented here.

Inspect |
With the patient in a sitting position, inspect the breasts visually. While inspecting,
look for:
- Visible masses (change in contour)
- Skin dimpling
- Nipple retraction
- Redness
|

Symmetry |
While generally symmetrical, many breasts are somewhat asymmetrical in respect to size,
shape, orientation, and position on the chest wall. |

Raise Arms |
Have her raise her arms while you continue to watch.
- An underlying malignancy can fix the skin in place. Raising the arms will accentuate
these changes.
|

Tighten Pectoralis Muscles |
Flex the pectoralis major muscles.
- A simple way to do this is have her place her hands on her hips and squeeze inward.
- With flexion of the underlying muscle, areas of breast tissue that are fixed in place
will move with the muscle, while the rest of the breast will not.
|

Palpate |
With the patient's arm raised over her head, palpate for lumps, masses or thickenings.
- Breast tissue is normally somewhat nodular or "lumpy," particularly in the
upper outer quadrant
|

Hand |
Use this portion of your hand to feel for lumps.
- The palm of the hand is too insensitive to detect subtle changes in breast
texture.
- The fingertips are too sensitive and will focus on the normal granularity of the breast
tissue rather than the more worrisome masses.
|
Use a Circular Motion |
Move your hand in a circular motion while pressing into the breast substance.
- Making these small circles will help you identify mass occupying lesions.
- With smaller breasts, palpation with one hand will give good results.
- When breasts are larger or pendulous, it may be useful to use two hands, compressing
the breast tissue between them.
|

Check Axilla |
Check the axilla for masses or palpable lymph nodes.
|

Supraclavicular Area |
The supraclavicular area can be an area of spread of breast malignancy.
- Check for any palpable masses or lymph nodes in this area.
- Then have the patient recline.
|

Reclining Palpation |
Sometimes, lumps or masses are better appreciated in the reclining or
semi-reclining position.
- One or two hands can be effectively used.
- The axilla can be checked in the reclining position or
semi-reclining position.
- The supraclavicular area can also be examined in the reclining
or semi-reclining position.
|
|

Check for Discharge |
Stripping the ducts toward the nipple will cause any secretions to be
expressed.
- In this case, the patient is lactating, so milk is expressed.
|
Self Breast Exam
Self breast exam comprises one portion of the triad of early detection of breast
abnormalities, the other two being professional breast exams and screening mammography.
This is appropriate, as most breast abnormalities are first discovered by the woman
herself.
Once a month, just after completing a menstrual flow, a woman should examine her
breasts. This can be done in the shower, but at least part of the exam should be done
while standing in front of a mirror.
 |
Inspect the breasts for:
- Skin changes
- Redness
- Visible bumps
- Nipple crusting
- Symmetry
|
 |
When raising her arms up, both breasts should rise evenly on the chest wall.
While raising her arms, she should watch closely for any skin dimpling or nipple
retraction.
|
 |
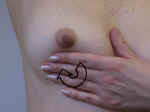
With her arm raised, she should feel for lumps with the opposite hand.
Most breast tissue is somewhat nodular. She is feeling for a "marble in a bag of
rice."
She should move her hand in small circles while compressing the breast tissue.
Then she should move to another area and perform the same small circular examination.
Many people find it easiest to move in a clockwise fashion to avoid missing any areas
of the breast.
|
 |
The same circular motion should be used to exam the armpit and the "tail" of
the breast that extends up into the armpit.
In the armpit, she is feeling for any breast lumps or lymph nodes. Enlarged lymph nodes
are about the size of a pencil eraser, but longer and thinner.
|
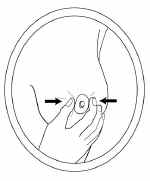 |
She should try to express nipple discharge by stripping the ducts towards the nipple.
Normally, there will be one or two drops of clear, milky or green-tinged secretions.
|
Mammography
Mammography is most often used as a screening technique for breast cancer.
Breast examinations detect most cancer, but will miss some, particular the very early
cancers that are too small to feel.
Mammograms are good at detecting some of these early cancers, but will miss others.
This means that breast exams and mammograms are complementary, each detecting problems the
other might miss.
Mammography looks for radio-opaque densities, microcalcifications, and disruption of
the normal breast architecture (parenchymal asymmetry).
For women without strong risk factors for breast cancer, screening mammography is often
done every other year between ages 40 and 50, and then annually after age 50.
Ultrasound
Mammography is very good at detecting radio-opaque changes, such as calcifications or
architectural distortion from a mass effect.
Ultrasound, in contrast, is very good at distinguishing cystic from solid masses. This
is probably most useful following mammographic findings of a benign-appearing,
non-palpable density, although it can also be used with palpable masses.
Breast Biopsy
Suspicious dominant breast masses are biopsied, as are suspicious areas found on
mammogram.
Commonly, this is done by fine-needle aspiration (FNA). A very thin needle is placed in
the suspicious area, suction applied, and multiple, tiny core samples taken.
Alternatively, open biopsy is sometimes necessary to remove all the suspicious tissue.
Supernumerary Breasts
Supernumerary breasts are relatively common. They are found along the "milk
line," extending from the axilla to the groin.
Most of them are not noticed clinically until pregnancy occurs. Then, under the
influence of the pregnancy hormones, the breasts enlarge in preparation for lactation. It
is at this time that soft swellings along the milk line occur, representing supernumerary
breasts. During lactation, the extra breasts may produce milk.
The two most common places for them are in the axilla and directly underneath the
normal breast.
These are not dangerous and are generally ignored. If they prove to be a cosmetic
problem, they can be removed surgically.
Supernumerary Nipples
More common than supernumerary breasts are supernumerary nipples. Like extra breasts,
these are located in the milk line and are not dangerous.
Unless they are large, they are usually not noticed until a pregnancy. At that time,
like the normal nipples, they enlarge and darken.
Inverted Nipples
Usually nipples point outward. Sometimes, they invert. When they persistently point
inwards, they are called inverted nipples. This can be unilateral or bilateral.
With stimulation and nipple erection, most inverted nipples will evert. Occasionally,
they remain inverted despite all efforts to evert them.
Other than for cosmetics, nipple inversion is not usually a problem. For
breast-feeding, most inverted nipples will evert. Even those that do not evert may still
function normally enough to allow for satisfactory infant nursing.
Adolescent Breast Problems
There is considerable individual variation in age at which this development occurs.
Asymmetrical breast growth during adolescence is the rule rather than the exception.
Reassurance is given that the asymmetry usually evens out by the time of full maturation.
Mammary hypertrophy can be a distressing symptom. Because growth and development
continues for a long time, surgical intervention, if contemplated is postponed until the
breasts are fully mature.
Breast masses in adolescents are essentially 100% benign. Because of this, surgery
(excisional biopsy or fine needle aspiration) is almost never warranted. Further, the
surgical disruption of architecture can be disfiguring as the breast continues to mature.
Pregnancy Changes
During pregnancy, a number of changes occur over time which prepare the breast for
lactation. These images demonstrate these changes:
- Early in the first trimester, the breasts and nipples become tender. The tenderness
persists until the end of the 1st trimester, at which time the tenderness disappears.
- By the end of the first trimester, enlargement of the breast and nipple is noticeable.
- By the third trimester, the breast and nipple have experienced further enlargement and
the Montgomery's glands around the periphery of the areola become more pronounced.
- The nipples gradually darken, becoming dark brown or black by full term.
Puerperal Mastitis
During lactation, breast infections (mastitis) are common. They are usually caused by
common skin bacteria (particularly staphylococcus) being introduced into the ductal system
through cracked nipples and the inoculation by the newborn suckling.
Clinically, these patients present with a rapid onset of unilateral breast tenderness,
redness, fever, and sometimes a thickening or mass.
Breast infections can be very aggressive with high fevers developing quickly. Immediate
treatment is important to keep an otherwise simple mastitis from developing an abscess,
requiring surgical drainage.
Good treatments include:
Continue to breast feed from the affected breast as drainage is important. Recurrent
infections are common.
Nipple Laceration
Occasionally, with vigorous nursing or newborn biting, a nipple laceration will occur.
This requires careful attention to avoid a major wound infection or breast abscess.
The nipple should be kept very clean and breast feeding on that side stopped to allow
the nipple to completely heal.
Instruct the patient to watch for any increasing tenderness or redness, which may be
evidence of a developing infection.
Routine administration of antibiotics are generally not necessary unless the laceration
is already infected or grossly contaminated.
Cyclic Breast Pain
During the days leading up to the menstrual flow, the breasts normally are somewhat
engorged and may be somewhat tender. Following the onset of menstrual flow, these changes
spontaneously resolve. If the tenderness is more than mild or is clinically bothersome, it
is called cyclic breast pain or mastodynia.
If examined during this time, these women also often have significantly
enhanced nodularity of the breast tissue. the combination of cyclic breast
pain and symmetrically thickened nodularity of the breast tissue is often
called fibrocystic disease (misnamed because it's not really a disease) or
fibrocystic breast changes.
While not dangerous, women with cyclic mastodynia find it annoying and in its most
severe form, interferes with some normal activities.
Some women find that by reducing or eliminating their intake of caffeine (coffee, tea,
cola drinks) and taking Vitamin E supplements (400
IU daily) has seemed to improve their symptoms. Whether such improvement is pharmacologic
or placebo in nature is still under debate.
Any pharmacologic approach that suppresses ovulation will be very helpful in treating
cyclic mastodynia. Among these, birth control pills are the simplest. Taking BCPs in the
usual fashion generally improves the pain significantly. For those who still experience
significant pain, continuous birth control pills will
usually suppress the pain completely.
Also effective, by virtue of ovulation inhibition, are depot
medroxyprogesterone acetate, Lupron, or Danocrine, the latter two usually justified only in
severe cases due to their significant side effects.
Non-cyclic Breast Pain
Among the common causes of non-cyclic breast pain are trauma, infection, and chest wall
pain underlying the breast tissue (muscle strain or overuse of the pectoralis major
muscle). Breast cancer rarely causes breast pain in the early stages and is not usually
suspected unless the symptoms persist. Hormonal causes include functional ovarian cysts
and pregnancy.
Women complaining of non-cyclic breast pain should have a careful examination and if
the pain persists, referral will likely be necessary.
Nipple Discharge
Normally, if the ducts are stripped toward the nipple, a drop or two of clear, milky,
or greenish-tinged liquid will appear. This is not considered nipple discharge.
Milk from a lactating woman considered normal.
If the nipples spontaneously leak discharge, staining the clothing, that is not normal,
nor is it normal to have bloody nipple secretions
Nipple discharge from both breasts indicates "galactorrhea." While a few post
partum women will continue to leak small amounts of milk for years following delivery,
galactorrhea in general indicates the need for a serum prolactin measurement and possibly
an MRI of the pituitary gland to look for prolactin-secreting pituitary adenomas.
Hypothyroidism can also cause this problem, although it is rare.
Athletes may experience small amounts of galactorrhea from constant rubbing of the
nipples against clothing. Frequent sexual stimulation of the breasts may have similar
effects. The serum prolactin measurement is best
made after a few days of non-stimulation of the breast. Even after a breast exam, it is
often helpful to wait 2 days before measuring the serum prolactin.
Persistent discharge from a single duct, particularly if bloody, rust-colored or
multicolored, suggests the presence of an intraductal lesion, such as a papilloma. While
these are often benign, they need further exploration with a general or breast surgeon.
Fat Necrosis
Fat necrosis presents as a breast mass with surrounding ecchymosis (bruise). It may be
tender and a history of breast trauma is identified in half the cases. Even when
significant trauma is not identified, it is felt to be the general cause of this
condition.
This benign condition is self-resolving, but is of clinical importance because it
mimics the dominant mass found in breast cancer.
Those cases with the typical presentation can be followed to make sure they completely
resolve. Those cases that are not typical or if there is any doubt, can have a fine needle
aspiration to confirm the diagnosis.
Paget's Disease
This crusty, flaking lesion is associated with an underlying breast malignancy,
invasive or in-situ. The appearance may be suggestive of Paget's disease, but the
diagnosis is generally confirmed by nipple biopsy.
The onset of the lesion is often so gradual that by the time it comes to the attention
of the physician, many months or years have passed since its' onset.
Treatment depends on the character and extent of the underlying lesion.
Breast Mass
If a dominant mass is found in the breast which persists through the menstrual cycle,
it is usually biopsied, either through fine needle aspiration or excisional biopsy,
depending on the clinical circumstances. In operational settings, this can wait a few
weeks, but should not wait much longer.
Suspicious masses (large, irregular, hard, fixed in place, with redness and dimpling of
the overlying skin and nipple retraction) are usually biopsied right away.
Most masses are benign, but for those found to be malignant, earlier intervention is
thought by many to lead to improved chances of successful treatment.
Breast Cyst
Breast cysts present as smooth, non-tender masses. They will often disappear over the
course of the menstrual cycle, but those that persist will need further evaluation.
Cyst aspiration is frequently attempted, using a small needle and syringe.
After aspiration of the cyst fluid is performed primarily to confirm the fact of the
cyst and to decompress it. Many physicians discard the cyst fluid unless it is bloody as
cyst fluid cytologic examination is felt to be of little value.
Following decompression of the cyst, the patient returns for periodic follow-up to look
for recurrence. Recurrent cysts in the same location are often subjected to excisional
biopsy or fine needle aspiration biopsy.
Fibroadenoma
These common, benign, solid, round or oval breast tumors are most common among women
ages 15-35. They are rubbery in consistency, mobile and non-tender. They rarely grow
larger than 2-3 cm.
The diagnosis is usually suspected on physical exam and confirmed with fine needle
aspiration or excisional biopsy. When found in teenagers, they are often simply watched
because of the very low risk of malignancy compared to the architectural disturbance
caused by excisional biopsy.
Breast Cancer
Breast cancer is a relatively common cancer, representing about 30% of all cancers in
women. In broad terms, treatment is successful in about 3 out of 4 patients in controlling
or eliminating the cancer. In about one out of four, the cancer proves fatal.
The risk of developing breast cancer increases steadily with increasing age. It is rare
among women under age 25 but affects nearly one in nine of those women reaching age 90.
A number of factors are associated with an increased of developing breast cancer,
including:
- Strong family history of breast cancer
- Menopause after age 55
- No term pregnancy prior to age 35
Despite the increased risk, most (about 80%) of breast cancer occurs in women not at
increased risk for developing breast cancer. For that reason, efforts at early detection
are not focused just on those with somewhat increased risks, but on all women. The primary
strategy involves a three-armed effort: Periodic (annual) professional breast examination,
monthly self-breast examination, and mammography at appropriate intervals.
Home
|




