|
1st Trimester Bleeding
Any bleeding during the first trimester of pregnancy is abnormal. The cause may
be trivial or serious, but it is always abnormal.
Bleeding during the first trimester is common. At least one-third of all
pregnant women will experience some degree of bleeding (perhaps only light
spotting) during this time. Half of those will ultimately lose the pregnancy,
while the other half will continue their pregnancy normally and without any
further problems.
 Clinical evaluation of women with first trimester bleeding involves looking
for evidence of: Clinical evaluation of women with first trimester bleeding involves looking
for evidence of:
Depending on the clinical circumstances, evaluation may include a history,
physical exam, and such laboratory tests as ultrasound,
quantitative HCG, and
progesterone.

Heavy bleeding from an incomplete
abortion
Abortion
Loss of a pregnancy during the first 20 weeks of pregnancy, at a time that the fetus
cannot survive. Such a loss may be involuntary (a "spontaneous" abortion), or it
may be voluntary ("induced" or "elective" abortion).
Miscarriage is the layman's term for spontaneous abortion, an unexpected 1st trimester
pregnancy loss. Since the term "spontaneous abortion" may be misunderstood by laymen, the
word "miscarriage" is sometimes substituted.
Abortions are further categorized according to their degree of completion. These
categories include:
-
Threatened
-
Inevitable
-
Incomplete
-
Complete
-
Septic
Such losses are common, occurring in about one out of every 6 pregnancies.
For the most part, these losses are unpredictable and unpreventable. About 2/3 are
caused by chromosome abnormalities incompatible with life. About 30% are caused by
placental malformations and are similarly not treatable.
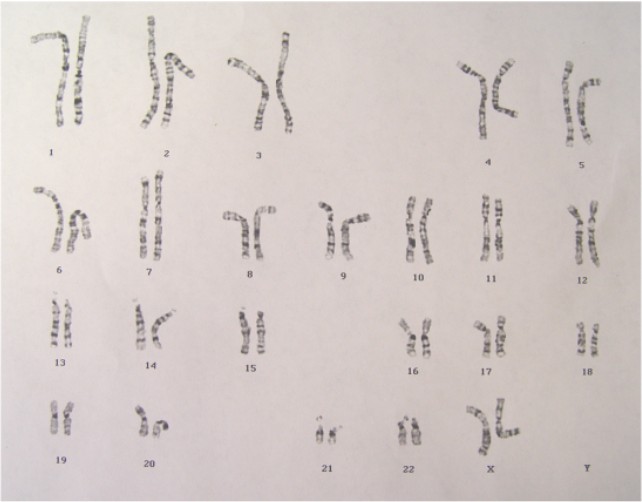
Normal 46XX female karyotype
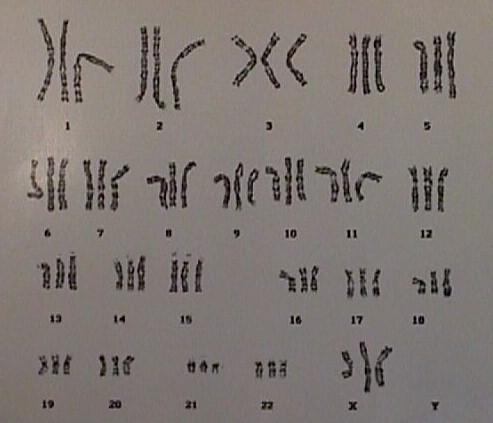
Triploidy
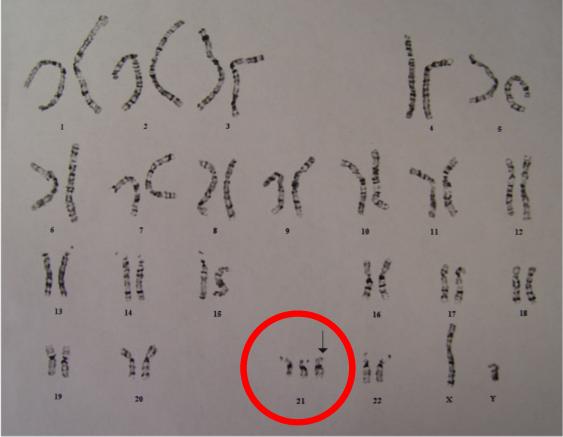
Trisomy 21 (extra #21 chromosome) in a
male (one X and one Y chromosome).
The remaining miscarriages are
caused by miscellaneous factors but are not usually associated with:
-
Minor trauma
-
Intercourse
-
Medication
-
Too much activity
Following a miscarriage, the chance of having another
miscarriage with the next pregnancy is about 1 in 6. Following two miscarriages in a row,
the odds of having a miscarriage with the next pregnancy is still about 1 in 6. After
three consecutive miscarriages, the risk of having a fourth is greater than 1 in 6, but
not very much greater.
Threatened
Abortion
A threatened abortion means the woman has experienced symptoms of bleeding or cramping.
At least one-third of all pregnant women will experience these symptoms. Half will go
on to abort spontaneously. The other half will see the bleeding and cramping disappear and
the remainder of the pregnancy will be normal. These women who go on to deliver their
babies at full term can be reassured that the bleeding in the first trimester will have no
effect on the baby and that you expect a full-term, normal, healthy baby.
Treatment of threatened abortion should be individualized. Many obstetricians recommend
bedrest in some form for women with a threatened abortion. There is no scientific evidence
that such treatment changes the outcome of the pregnancy in any way, although some women
may feel better if they are at rest. Other obstetricians feel that being up and active is
psychologically better for the patient and will not change the risk of later miscarriage.
Among these active women, strenuous physical activity is usually restricted, as is
intercourse.
|
Incomplete
Abortion
With an incomplete abortion, some tissue remains behind
inside the uterus.
These typically present with continuing bleeding,
sometimes very heavy, and sporadic passing of small pieces of pregnancy tissue.
Ultrasound may reveal the presence of
identifiable tissue within the uterus. Serial quantitative HCG levels can be measured if
there is doubt about the completeness of a miscarriage.
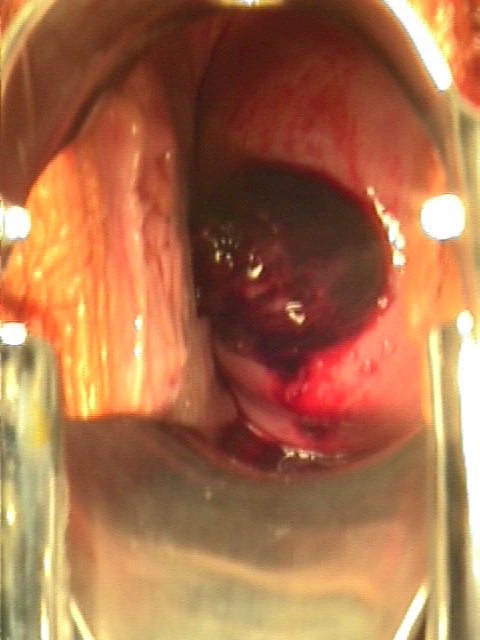
Incomplete abortion with products of
conception passing through the dilated cervical os
Left alone, many of these cases of incomplete abortion
will eventually resolve spontaneously, but so long as there are non-viable pieces of
tissue inside the uterus, the risks of bleeding and infection continue.
Treatment consists of converting an incomplete abortion
into a complete abortion. Usually, this is done with a D&C (dilatation and curettage).
This minor operation can be performed under local anesthesia and takes just a few minutes.
Alternatively, bedrest and oxytocin, 20 units (1 amp) in 1 Liter of any
crystalloid IV fluid at 125 cc/hour may help the uterus contract and expel the remainder
of the pregnancy tissue, converting the incomplete abortion to a complete abortion.
Alternatively, ergonovine 0.2 mg P.O. or IM three times daily for a few days may be
effective.
If fever is present, broad-spectrum antibiotics are wise.
Any tissue fragments visibly protruding from the cervical
os can be grasped with a ring or dressing forceps and gently pulled straight out. This
simple and safe procedure will have a beneficial effect on the bleeding.
Inevitable
Abortion
Inevitable abortion means that a miscarriage is destined
to occur, but no tissue has yet been passed. This is sometimes called a "missed
abortion."
This diagnosis is best made by
ultrasonic visualization of the fetal heart and noting no movement.
Alternatively, demonstrating no growth of the fetus over a one week
period in early pregnancy confirms an inevitable abortion. Falling
levels of HCG are an ominous sign and strongly suggest the pregnancy is
no longer living.
Two alternative approaches are
considered for an inevitable abortion: D&C or awaiting a spontaneous
abortion. Each approach has its own merits and limitations:
-
Awaiting a spontaneous abortion offers the benefit of
avoiding surgery, but commits the patient to a day or more of heavy bleeding and cramping.
A few of these women will experience an incomplete abortion and will need to have a
D&C anyway.
-
Performing a D&C has the benefit of quickly
resolving the issue of a missed abortion, but commits the patient to a surgical procedure
which carries some risks.
Septic
Abortion
During the course of any abortion, spontaneous or induced, infection may set in.
Such infections are characterized by fever, chills, uterine tenderness and
occasionally, peritonitis. The responsible bacteria are usually a mixed group of Strep,
coliforms and anaerobic organisms. These patients display a
spectrum of illness, ranging from mild, to very severe.
Usual treatment consists of bedrest, IV antibiotics, uterotonic agents, and complete
evacuation of the uterus. If the patient does not respond to these measures and is
deteriorating, surgical removal of the uterus, tubes and ovaries may be life-saving.
Evacuation of the uterus can be initiated with oxytocin, 20 units (1 amp) in 1 Liter of
any crystalloid IV fluid at 125 cc/hour or ergonovine 0.2 mg P.O. or IM three times daily.
If the patient response is not favorable, or if the patient is quite
ill, D&C is the next step.
IV antibiotics should be started immediately. Among many good choices for
this treatment are:
Another good choice could be:
|

{kind=link}