|
After delivery of the baby, the placenta
normally detaches from the inside of the uterus and
is expelled, often with additional pushing efforts by the mother. Normally this
occurs within a few minutes of delivery of the baby, but may take as long as an hour.
 The four signs of placental separation are: The four signs of placental separation are:
-
Apparent lengthening of the visible portion of the umbilical
cord.
-
Increased bleeding from the vagina.
-
Change in shape of the uterus from flat (discoid) to round
(globular).
-
The placenta being expelled from the vagina.
Commonly, after about 30 minutes of waiting or if there is increased
bleeding without evidence of placental separation, a manual removal of the placenta is
undertaken. Anesthesia (regional or general) is typically used for this as manual removal
can cause considerable abdominal cramping. Sometimes,
IV narcotic analgesia
will prove helpful in relieving this discomfort
Manual Removal of the Placenta
One hand is inserted through the vagina and into the uterine cavity.
-
Insert the side of your hand in between the placenta and the
uterus. You may need to push through the placental membranes to
accomplish this.
-
Using the side of your hand, sweep the placenta off the uterus.
-
After most of the placenta has been swept off the uterus, curl
your fingers around the bulk of the placenta and exert gentle
downward and outward traction. You may need to release the placenta
and then re-grab it.
-
Then pull the placenta through the cervix. Most placentas can be
easily and uneventfully removed in this way. A few prove to be
problems.
Placenta Accreta and Percreta
When you manually remove the placenta, be prepared to deal with an abnormally adherent
placenta (placenta accreta or placenta percreta). These abnormal attachments may be
partial or complete.
-
If partial and focal, the attachments can be manually broken and the placenta removed.
It may be necessary to curette the placental bed to reduce bleeding. Recovery is usually
satisfactory, although more than the usual amount of post partum bleeding will be noted.
-
If extensive or complete, you probably won't be able to remove the placenta in other
than handfuls of fragments. Bleeding from this problem will be considerable, and the
patient will likely end up with multiple blood transfusions while you prepare her for a
life-saving, post partum uterine artery ligation or hysterectomy. If surgery is not
immediately available, consider tight uterine and/or vaginal packing to slow the bleeding
until surgery is available.
|

Separate the placenta from the uterus with a
sweeping motion
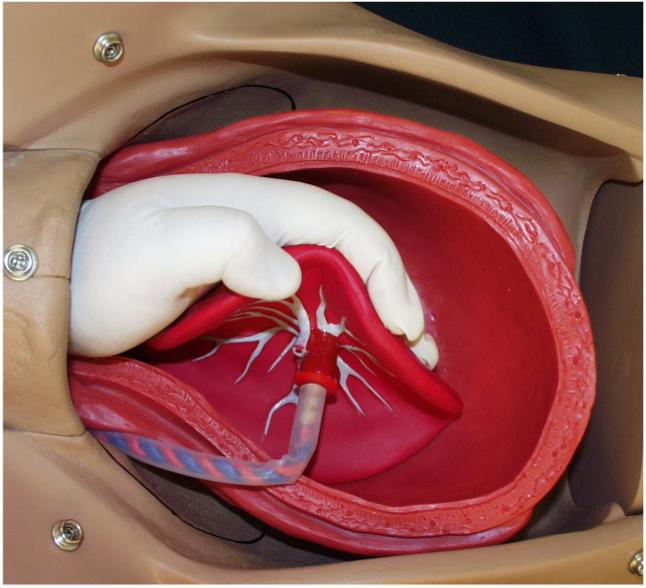
After the placenta is mostly separated, curl
your palm around the bulk of it.

Continue to grasp the placenta as you remove it
from the uterine cavity.
|