|
Shoulder Dystocia
Excessive Traction
· Episiotomy · Macrobert's
Maneuver · Suprapubic Pressure · Deliver
Posterior Arm · Screw Maneuver
Shoulder dystocia means difficulty with delivery of the fetal shoulders.
Watch a video showing shoulder dystocia.
|
Shoulder Dystocia
Excessive Downward Traction
Gentle Downward Traction

MacRobert's Maneuver
Suprapubic Pressure

Suprapubic Pressure

Delivery of Posterior Arm
Unscrewing Shoulder

Continue 360 Degrees
Shoving Scapulas Saves Shoulders |
In a
spontaneous vaginal delivery, after the baby’s head passes through the birth
canal, the baby’s shoulders normally rotate underneath the pubic bone and then
are expelled with the fetal torso and extremities. In a few cases, the shoulder
fails to spontaneously pass beneath the pubic symphysis, catching on the pubic
bone.
Shoulder dystocia is a dangerous condition because:
1. If it is not relieved, it can lead to fetal
death, and
2. There is a significant risk of injury to the
nerves in the neck from stretching or tearing.
3. The
condition and maneuvers to relieve it are associated with an increased risk of
fractures of the clavicle and humerus.
It
probably occurs to some degree in between 1% and 5% of all deliveries, depending
on the patient population, the experience of the operator, definitional
differences, and the accuracy of reporting.
It
would likely occur more often, but the maternal pelvis is somewhat stretchy, the
fetus is somewhat compressible, most deliveries are of normal size and shaped
infants through normal size and shaped pelvises.
Although shoulder dystocia is more common among women with gestational diabetes
and those with very large fetuses, it can occur with babies of any size.
Unfortunately, it cannot be predicted or prevented, so birth attendants should
be prepared to deal with this issue, even if the patient is considered low risk.
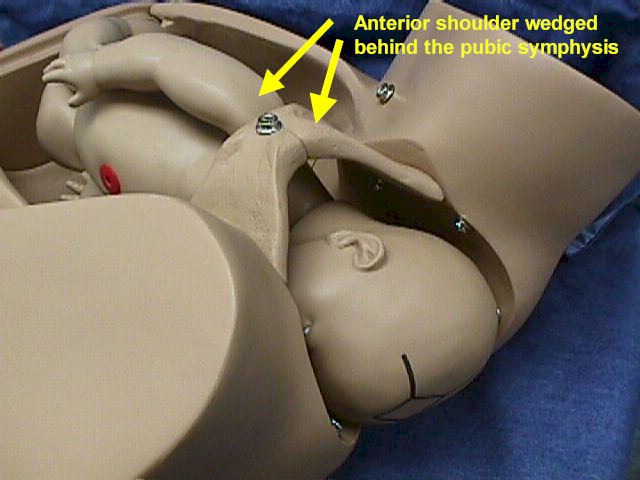
Suspect a shoulder dystocia if, after delivery of the head, the fetal head
partially withdraws back into the birth canal. This is called the "Turtle Sign".
It occurs because the anterior shoulder is stuck behind the pubic symphysis.
Insert one finger vaginally, and you will be able to feel the shoulder stuck
behind the pubic bone.
In
more severe cases, the posterior shoulder may be stuck at the level of the
sacral promontory.
You
should immediately call for extra help since many of the maneuvers you will need
to perform will require more than a single person, anesthesia and newborn
resuscitation and support may be needed.
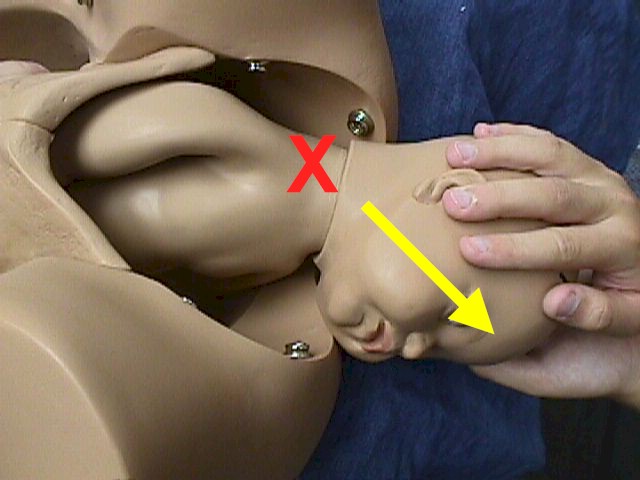
Avoid Excessive Downward Traction
Try to avoid
applying excessive downward traction to the baby's head. The nerves of the brachial plexus course through the neck
and into the arm. Stretching or tearing of these nerves can cause or aggravate
an injury with serious consequences to the baby.
While most of these nerve injuries heal spontaneously and completely, some do
not.
Generous Episiotomy
A generous
episiotomy can be helpful. If a spontaneous laceration has occurred, or if the
perineum is very stretchy and offers no obstruction, then it is not necessary to
also perform an episiotomy. However, if there is any soft tissue obstruction or
if the perineum interferes with your ability to perform extraction maneuvers, it
is wise to place a large episiotomy, a second episiotomy, or extend a perineal
laceration with scissors to obtain more room. Some physicians will perform an
intentional 4th degree extension in order to facilitate delivery. The 4th degree
extension can usually be easily repaired without any long-term consequences for
the mother and provides excellent exposure for the delivery.
Gentle downward traction can be attempted initially to try to free the shoulder, although some physicians
prefer to not exert any downward traction to facilitate the delivery.
If
gentle downward traction has no effect, do not exert increasing pressure.
Instead, try some alternative maneuvers to free the shoulder.
McRobert's Maneuver
The McRobert's Maneuver involves flexing the maternal thighs tightly against the mother’s abdomen. This
can be done by the woman herself or by assistants.
By
performing this maneuver,
-
The axis of the birth canal
is straightened, allowing a little more room for the shoulders to slip
through, and
-
The pressure of the mother's
thighs on her abdomen provides the equivalent of suprapubic pressure to
dislodge the shoulder from behind the pubic bone.
With the patient in the McRobert's position, you can try gentle downward traction again. If gentle traction has no effect, stop the traction and try another
maneuver.
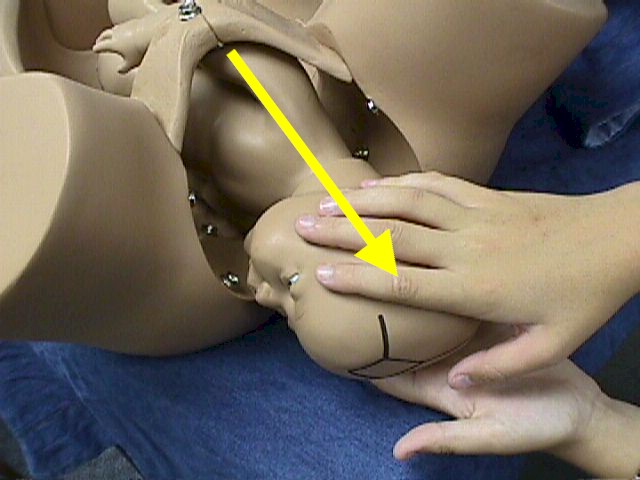
Suprapubic Pressure
Suprapubic pressure can be applied to drive the fetal shoulder downward, clearing the pubic bone.
It
is usually easiest to have an assistant apply this downward pressure while you
apply coordinated, gentle downward traction and the mother bears down.
Sometimes, the suprapubic pressure is more effective if applied in a somewhat
lateral direction, rather than straight down. This tends to nudge the shoulder
into a more oblique orientation, which in general provides more room for the
shoulder. Usually, this lateral pressure is directed so as to shove the baby’s
shoulder towards its’ breastbone, but any direction of force that is effective
in moving the baby’s shoulder away from the entrapped anterior-posterior
orientation into a more oblique or lateral orientation can give good results.
Gentle downward traction on the fetal head in combination with this suprapubic
pressure, maternal pushing efforts and MacRobert's position may relieve the
obstruction. If not, stop the pushing and pulling efforts, and try another
maneuver.
Deliver the Posterior Arm
Often, by the time the fetal head has delivered, the posterior arm has entered
the hollow of the sacrum. By reaching in posteriorly and sweeping the arm up and out of the
birth canal, enough
additional space will be freed to allow the anterior shoulder to clear the pubic
bone.
This
description makes the maneuver sound easier than it is. Because of limited
visibility and space, this maneuver is sometimes difficult or impossible.
Identify the posterior shoulder and follow the fetal humerus down to the elbow.
Then you can identify the fetal forearm. Grasping the fetal wrist, draw the arm
gently across the chest and then out. Once the posterior arm has delivered, you
can try each of the previous maneuvers again as you have reduced the bisacromial
diameter and it will be easier for the anterior shoulder to descend.
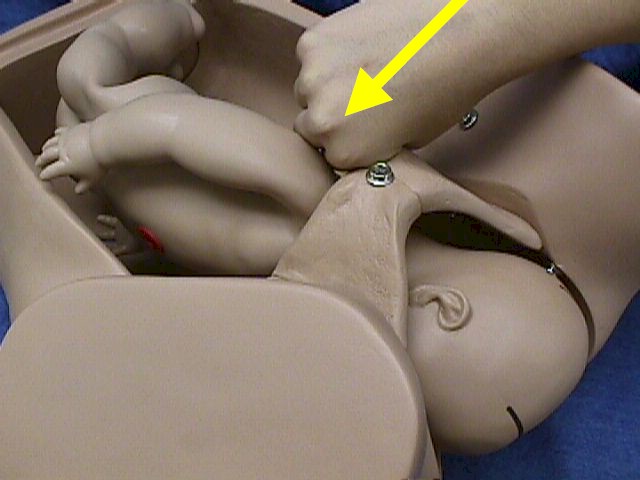
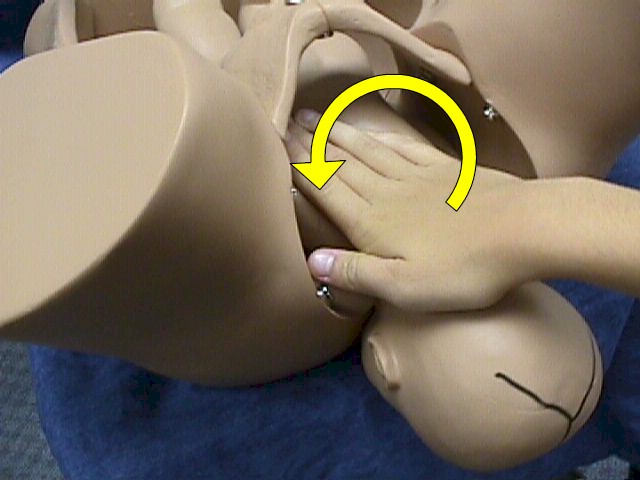
Screw Maneuver
If you
try to remove an electric light bulb by simply pulling on it, it won't work. If,
however, you unscrew the light bulb, it comes out relatively easily.
The
concept of unscrewing the light bulb can be applied to shoulder dystocia
problems.
The image shown here shows pushing the anterior shoulder in a counterclockwise direction. As the baby
rotates, the posterior shoulder comes up outside of the subpubic arch. At the
same time, the stuck anterior shoulder is brought posteriorly into the hollow of
the sacrum. As the rotation continues a full 360 degrees, both shoulders are
rotated (unscrewed) out of the birth canal.
It
is sometimes easier to perform this maneuver with your hand on the posterior
shoulder, rotating it up. If you have enough room in the pelvis, using both your
hands, one on the posterior shoulder and one on the anterior shoulder can
produce excellent results.
In
cases where both the anterior and posterior shoulders are stuck, the baby may
need to be rotated twice. The first rotation brings a shoulder down into the
hollow of the sacrum, while the second rotation brings that shoulder up and
outside the subpubic arch.
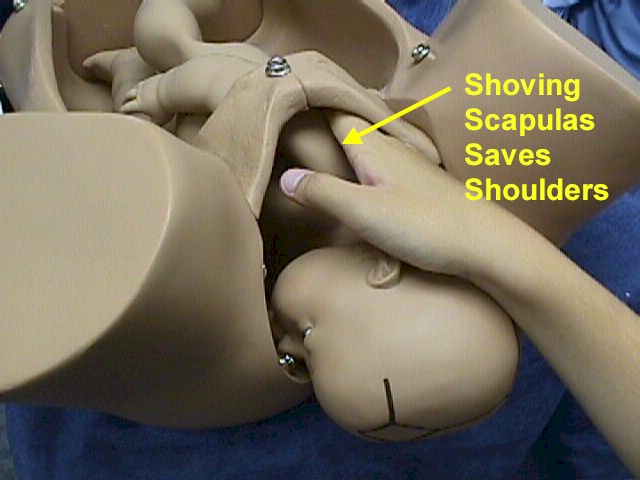
Shoving Shoulders Saves Scapulas
Two variations on the unscrewing maneuver include:
-
Shoving the
shoulder towards the fetal chest, which compresses the shoulder-to-shoulder
diameter, and
-
Shoving the
anterior shoulder rather than the posterior shoulder. The anterior shoulder
may be easier to reach and simply moving it to an oblique position rather than
the straight up and down position may be sufficient
If
these maneuvers have failed, it is appropriate to repeat them in various
combinations, and with increasing forcefulness. While the increased forcefulness
may increase the risk of shoulder injury, the baby must ultimately be delivered
or it will die.
There are a few other maneuvers that are infrequently used.
Fundal Pressure
Applying fundal pressure in coordination with other maneuvers may, occasionally,
be helpful. Applied alone, it may aggravate the problem and increase the risk of
injury by further impacting the shoulder against the symphysis. You also run the
risk of uterine rupture if the fundal pressure is applied too vigorously or at
the wrong time. For these reasons, many obstetricians recommend avoiding fundal
pressure entirely.
Zavenelli Maneuver
Another infrequently-used technique to resolve shoulder dystocia is cephalic
replacement of the fetal head, followed by cesarean section. The fetal head is
flexed and pushed back up into the birth canal and held in place. The mother is
transported to an operating room, and a cesarean section performed. Generally
good results have been reported from a small number of cases in which this
maneuver has been performed.
Clavicular Fracture
Intentional fracture of the baby’s clavicle has been recommended in the past as
a way of narrowing the bisacromial diameter. A fractured clavicle in a newborn
usually heals well without long-term consequences and generally poses less of a
threat to the newborn than a brachial plexus nerve injury. That said, it is not
so easy to intentionally fracture a clavicle. I’ve tried to fracture a clavicle
several times during my career, but without success. At the same time, I have
inadvertently fractured several clavicles during my 30 years as an obstetrician.
Despite careful attention to detail and skillful performance of these maneuvers,
some babies will still sustain injury. No maneuver, no matter how skillfully
performed, can prevent all injuries. But the best chance for avoiding injuries
comes when shoulder dystocia is approached in a careful, systematic way, with
progressive increases in the forcefulness of the maneuvers, until just the right
combination of just the right forces delivers the baby.
|
