Prolapsed Umbilical Cord
 If a portion of the umbilical cord comes out of the cervix or vulva ahead of the fetus,
this is called a prolapsed umbilical cord. If a portion of the umbilical cord comes out of the cervix or vulva ahead of the fetus,
this is called a prolapsed umbilical cord.
This can be a big problem for the fetus
in a number of ways:
-
If the umbilical vein is obstructed, but the arteries are still
patent, then the fetus will continue to pump blood out to the
placenta but get nothing in return. This will lead fairly rapidly to
hypoxia (no fresh oxygen coming in), and hypovolemia (shock, from
reduction on available blood volume).
-
if the cord is totally compressed, hypoxia will develop
relatively quickly, and be aggravated by the bradycardia that
accompanies the obstruction of umbilical arteries.
None of this is good.
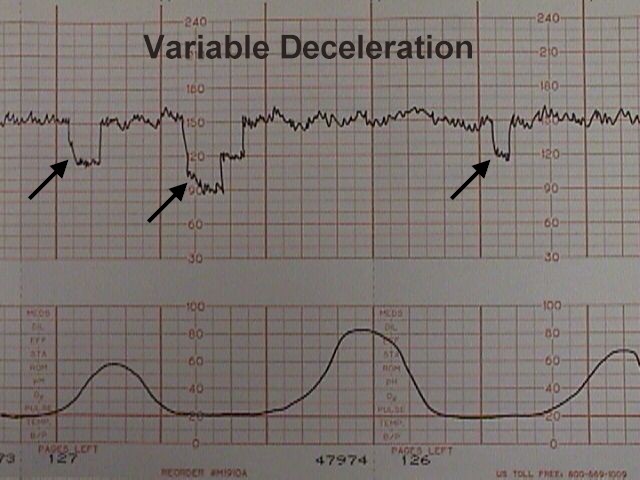
Prolapsed umbilical cords are often preceded by variable
decelerations of the fetal heart rate, demonstrated on the electronic
fetal monitor. Whenever these appear (and have not previously been
seen), it is a good idea to examine the pelvis for evidence of a
prolapsed cord. Whenever membranes rupture, check to make sure there is
no sign of a prolapsed cord.
 Once the cord is prolapsed, immediate delivery is the best solution. Once the cord is prolapsed, immediate delivery is the best solution.
Put the mother in the knee-chest position and use your hand in her
vagina to elevate the fetal head back up into the uterus. This action
may relieve enough pressure on the umbilical cord that oxygen can still
get through to the baby. I wouldn't be too reassured by feeling a normal
pulse in the umbilical cord between your fingers. The umbilical vein
could still be obstructed even with normal arterial pulsations.
Consider giving Terbutaline
0.25 mg SQ to stop her contractions, relieving pressure on the cord.
Transport the mother in the knee-chest position and you with your
hand elevating the fetal presenting part to the cesarean section room.
If, on arrival, the baby is immediately deliverable vaginally (with
forceps, vacuum extractor, etc.), then that is a safe approach. If the
fetus is not immediately deliverable, then proceed with cesarean
section.
If the cord has stopped pulsating, then the likelihood is that the
fetus has died. Cesarean section at this point will not change the
long-term outcome, and vaginal delivery should usually be continued.
|
