Premature Rupture of Membranes
Most women will rupture their membranes during labor. If membranes rupture prior to the
onset of labor, this is called premature rupture of the membranes, or PROM.
The obstetrical significance of PROM is that:
-
Labor needs to begin promptly or infection will develop with bacteria
ascending through the birth canal, and
-
In some cases of PROM, the reason the membranes rupture prematurely is
because there is an established infection which has weakened the
membranes.

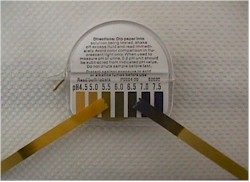
Nitrazine Positive |
Confirmation of PROM is optimally made via a sterile speculum examination,
although at full term, with obvious leakage of amniotic fluid from the vagina,
a simple pelvic exam will be expeditious. Look for:
-
Gross leakage of clear fluid from the cervical os.
-
Pooled amniotic fluid in the vagina
-
Nitrazine positive fluid
-
Ferning (fluid dried on a glass slide forms crystals)
Obtain a culture of the fluid. Rarely, there is a strong clinical
suggestion that membranes are ruptured, but there is no fluid in the vaginal
vault. In these unusual circumstances, amniocentesis may need to be performed,
with injection of sterile dye, to see if it appears in the vagina, confirming
ROM. Alternatively, a swab of the upper vagina can be sent for Nile Blue
Sulfate staining, to look for fetal fat cells.
If the pregnancy is at full term and there is no evidence of infection, no
treatment is necessary initially, because most women will go into spontaneous
labor within the next 6 hours. After 6 hours of rupture, or in the face of
infection or other pressing clinical circumstance, labor can be induced.
Unless infection is evident, antibiotics are not helpful, until the patient is
in labor and membranes have been ruptured >12 hours. In this case Group B Strep prophylaxis is a wise course.
When PROM occurs remote from term, two basic approaches can be taken:
-
Induce
labor, or
-
Wait for the fetus to mature further.
There are pros and cons to each of these approaches. The best decision will
frequently hinge on individual clinical circumstances. This decision is best
made in consultation with a definitive care facility. If there is evidence of chorioamnionitis, antibiotics are started and labor and delivery are
facilitated, regardless of gestational age. If chorioamnionitis is not
present, antibiotics are not helpful and are generally withheld. Following the
mother's WBC and temperature, and the fetal
baseline heart rate are useful in detecting the earliest signs of chorioamnionitis. The WBC, normally slightly elevated during pregnancy, may
show a steady increase. The combination of an elevated WBC, elevated maternal
temperature and fetal tachycardia suggests the presence of chorioamnionitis.
|

{kind=link}